Rotator Cuff Repair: Instruments & Implants Explained
Rotator cuff tears are among the most common and clinically consequential shoulder injuries in orthopedic practice. Whether caused by acute trauma or gradual degenerative wear, these tears – affecting one or more of the four rotator cuff tendons – can produce significant pain, weakness, and functional loss if left untreated. For the majority of full-thickness and symptomatic partial-thickness tears, arthroscopic repair is now the gold standard.
Understanding the shoulder arthroscopy essentials that underpin a successful repair – the instruments, the implants, and the decision-making framework behind each – is foundational knowledge for any surgeon performing these procedures. This article breaks down the complete picture.
Understanding the Rotator Cuff: A Brief Anatomical Overview
The rotator cuff comprises four muscles and their tendons: the supraspinatus, infraspinatus, teres minor, and subscapularis. Together they stabilize the glenohumeral joint, control rotation, and generate the force required for overhead and throwing activities. The supraspinatus is by far the most frequently torn, particularly at its critical zone of relative avascularity near the greater tuberosity footprint.
Tear classification – partial versus full-thickness, small versus massive, retracted versus mobile – directly drives both the surgical strategy and the implant selection. A surgeon who masters shoulder arthroscopy essentials must be equally fluent in anatomy, tear classification, and the biomechanical principles of tendon-to-bone repair.
Essential Arthroscopic Shoulder Instruments
Visualization and Portal Instruments
Arthroscopic shoulder instruments for rotator cuff repair begin with the arthroscope itself – typically a 4 mm, 30-degree lens providing wide-angle visualization of the subacromial space, bicipital groove, glenohumeral joint, and rotator cuff footprint. A high-definition camera system and a consistent light source are non-negotiable for accurate tissue assessment and safe anchor placement.
Cannulas and switching sticks maintain working portals and allow smooth instrument exchanges throughout the procedure. In rotator cuff repair, multiple portals are often required – posterior, anterosuperior, and lateral – and maintaining access to all three without portal compromise is an important intraoperative skill.
Tissue Preparation Tools
Before any implant is placed, the tendon and the greater tuberosity footprint must be properly prepared. Key instruments at this stage include:
- Motorized Shaver: Removes bursal tissue, inflammatory synovium, and ragged tendon edges to improve visualization and create a clean repair surface.
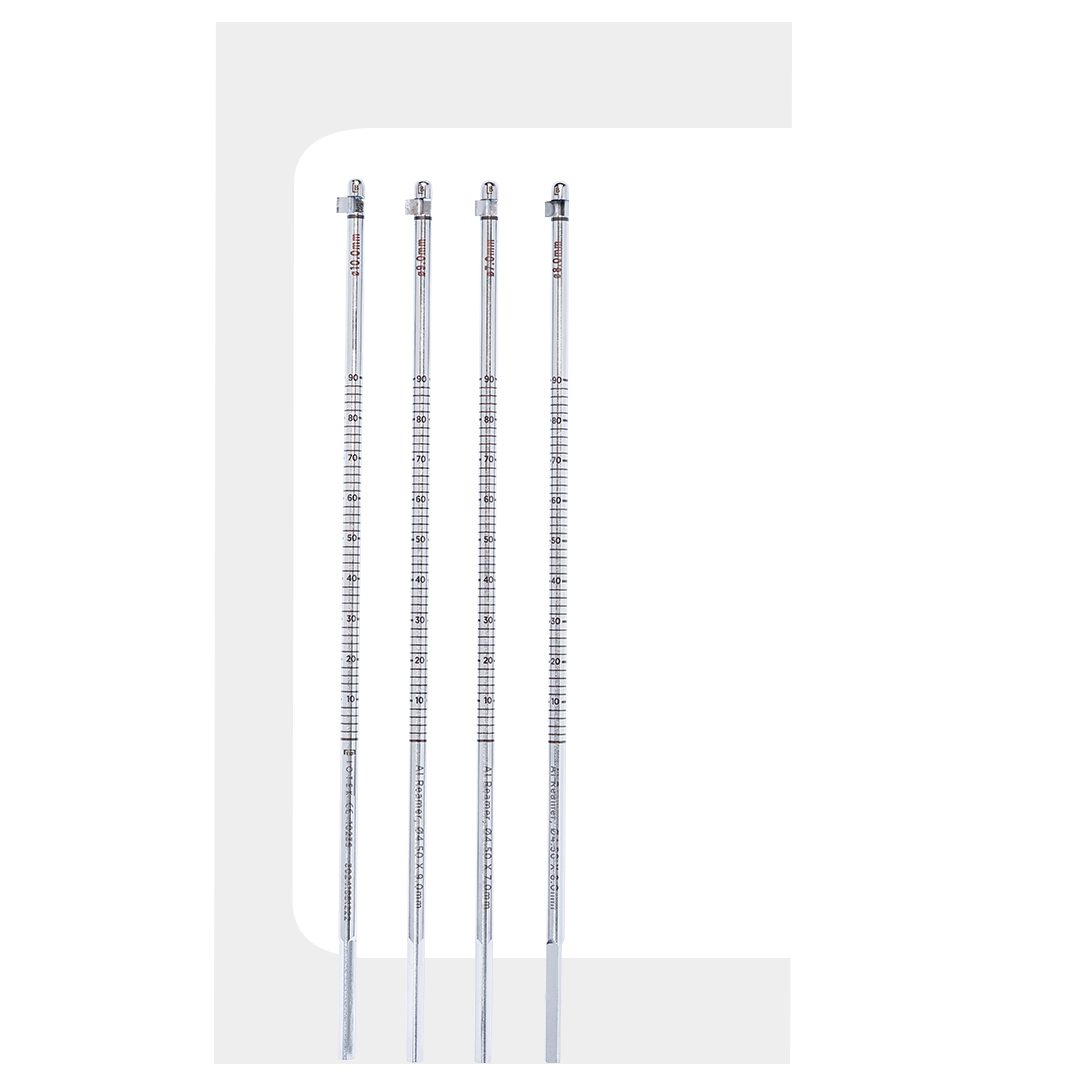
- Burr: Decorticates the greater tuberosity footprint to create a bleeding bone bed that supports tendon-to-bone healing through fibrovascular ingrowth.
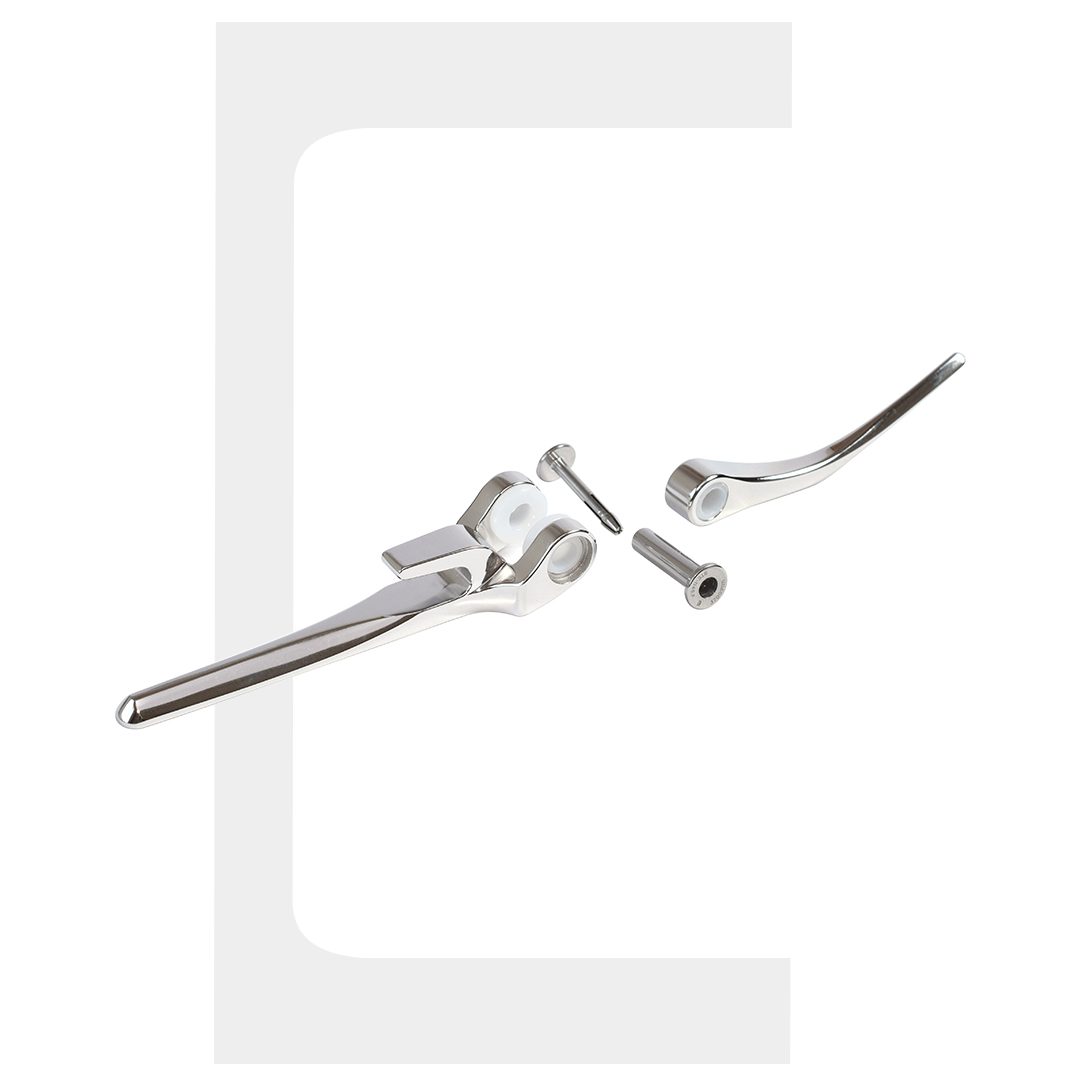
- Tissue Grasper: Assesses tendon mobility and positions the torn edge for anchor placement. Critical for determining whether a single-row or double-row construct is appropriate.
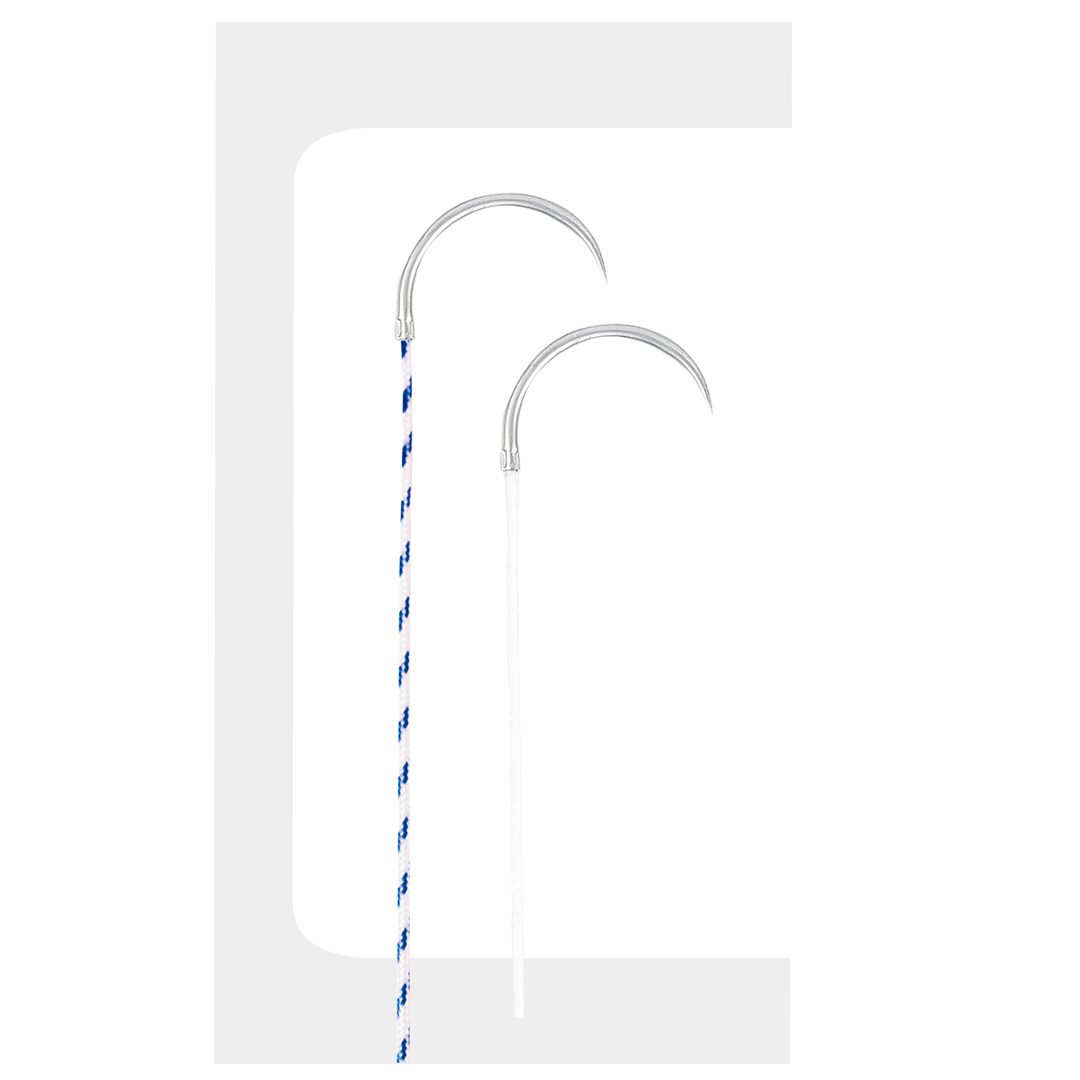
- Suture Passer: Shuttles suture through tendon tissue under direct visualization. Accuracy here determines mattress suture configuration quality and ultimately repair integrity.
Implants for Rotator Cuff Repair: What Matters Most
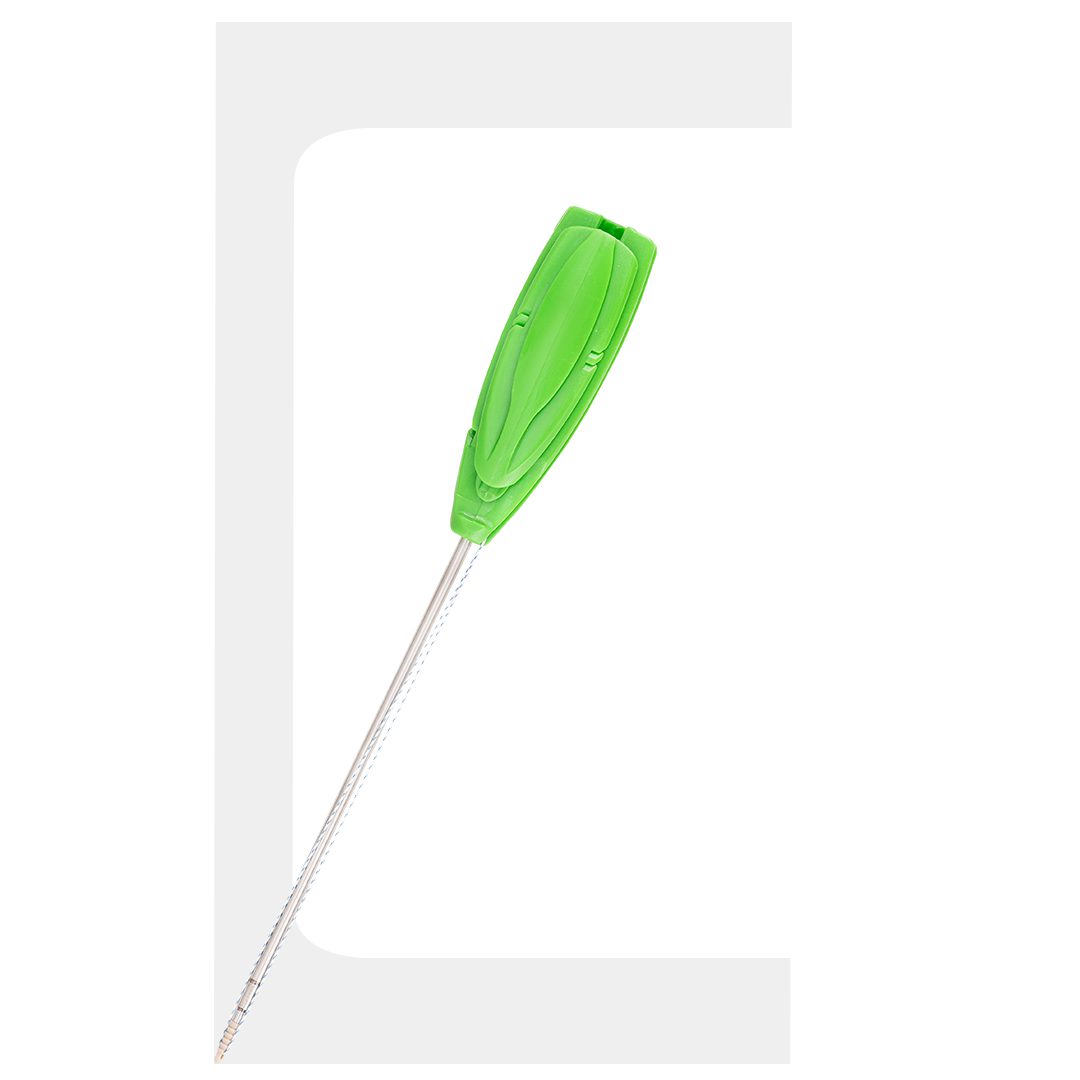
Suture Anchors: The Core Fixation Device
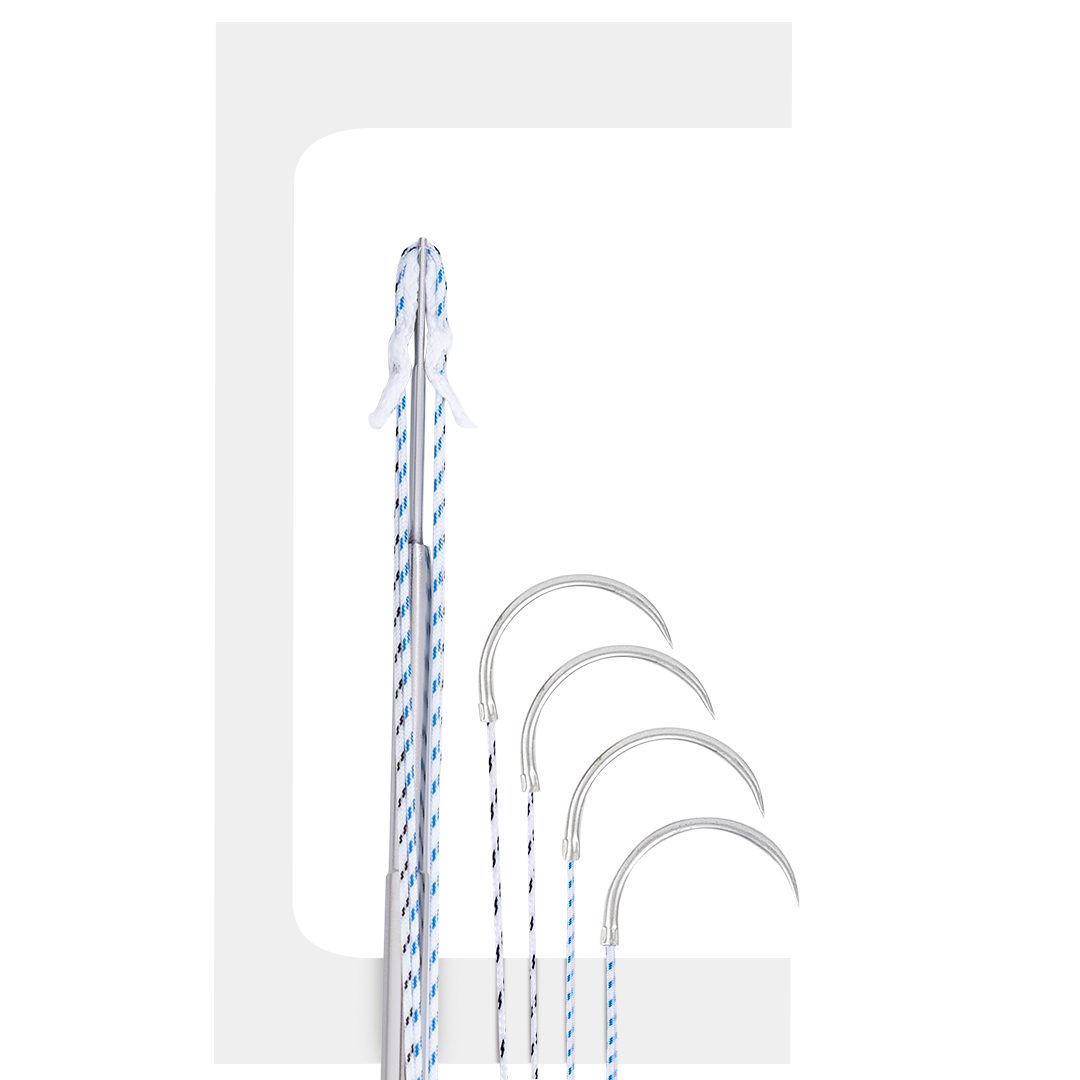
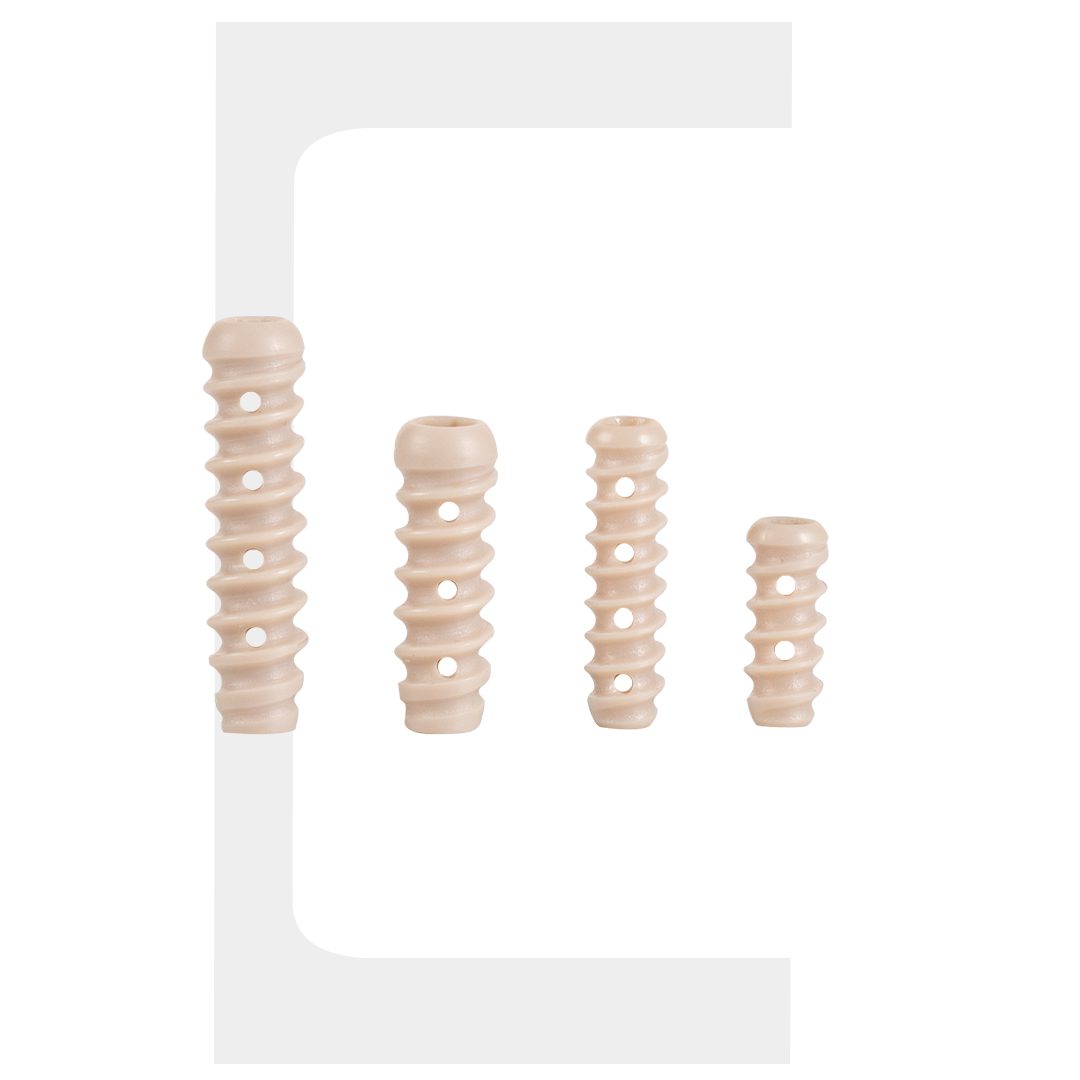
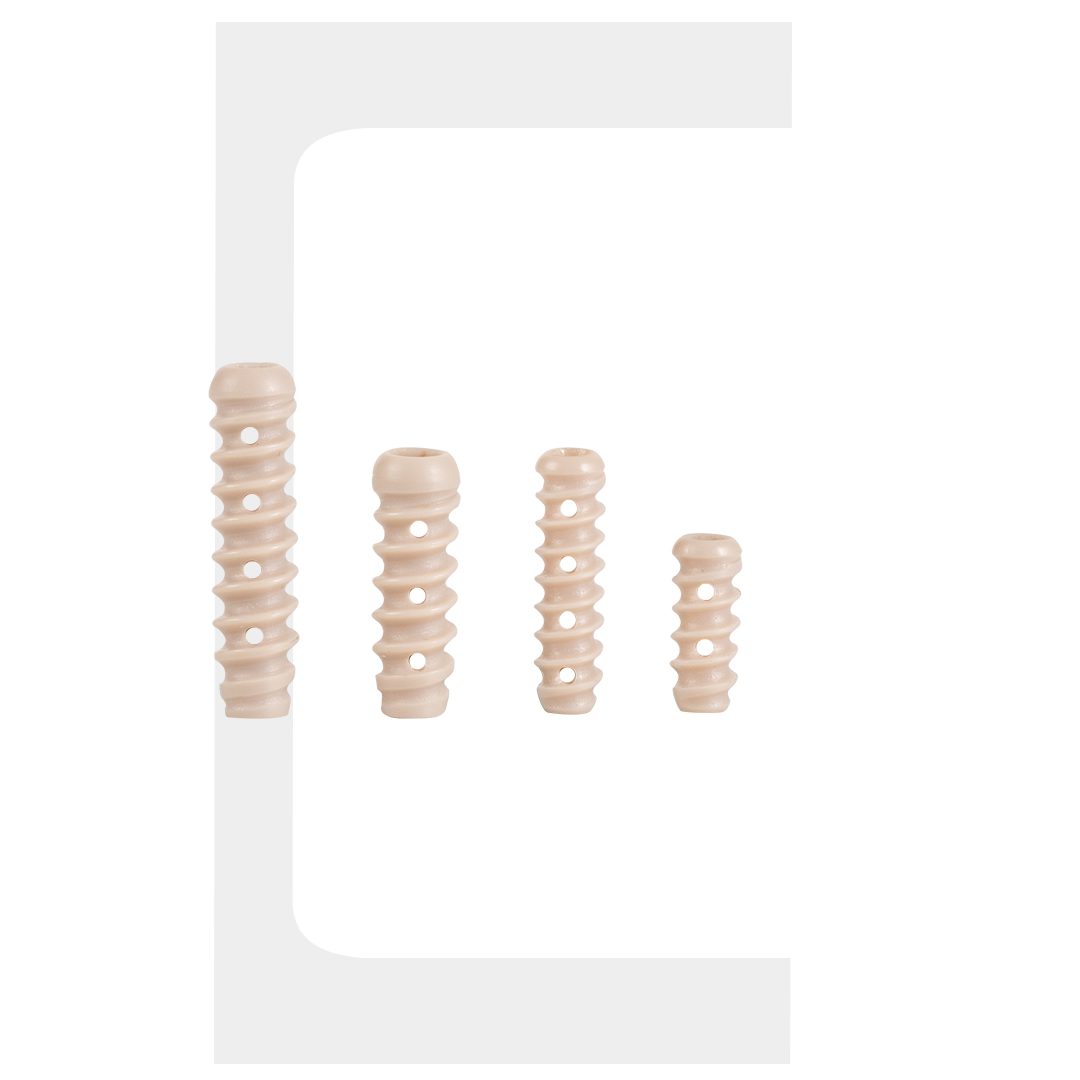
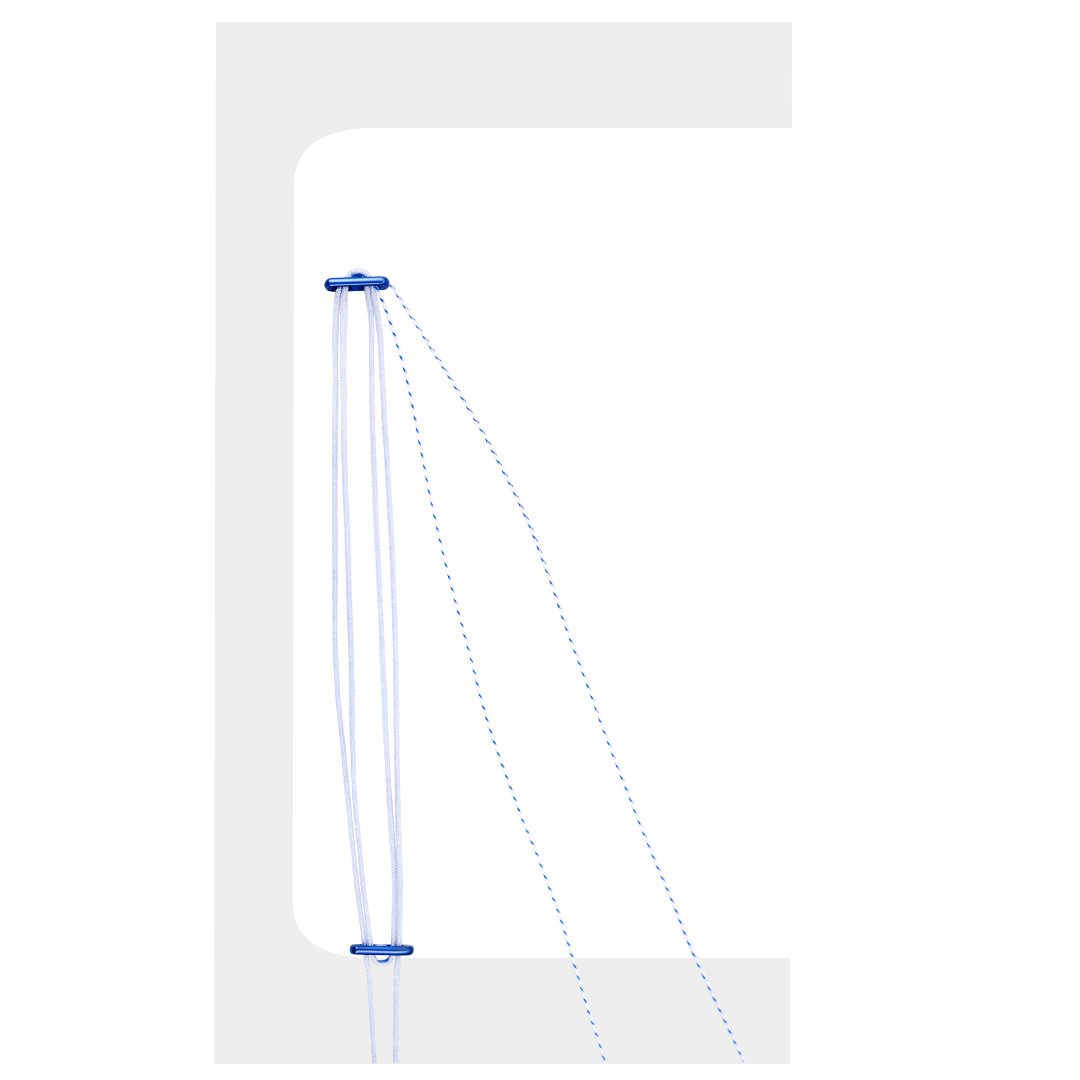
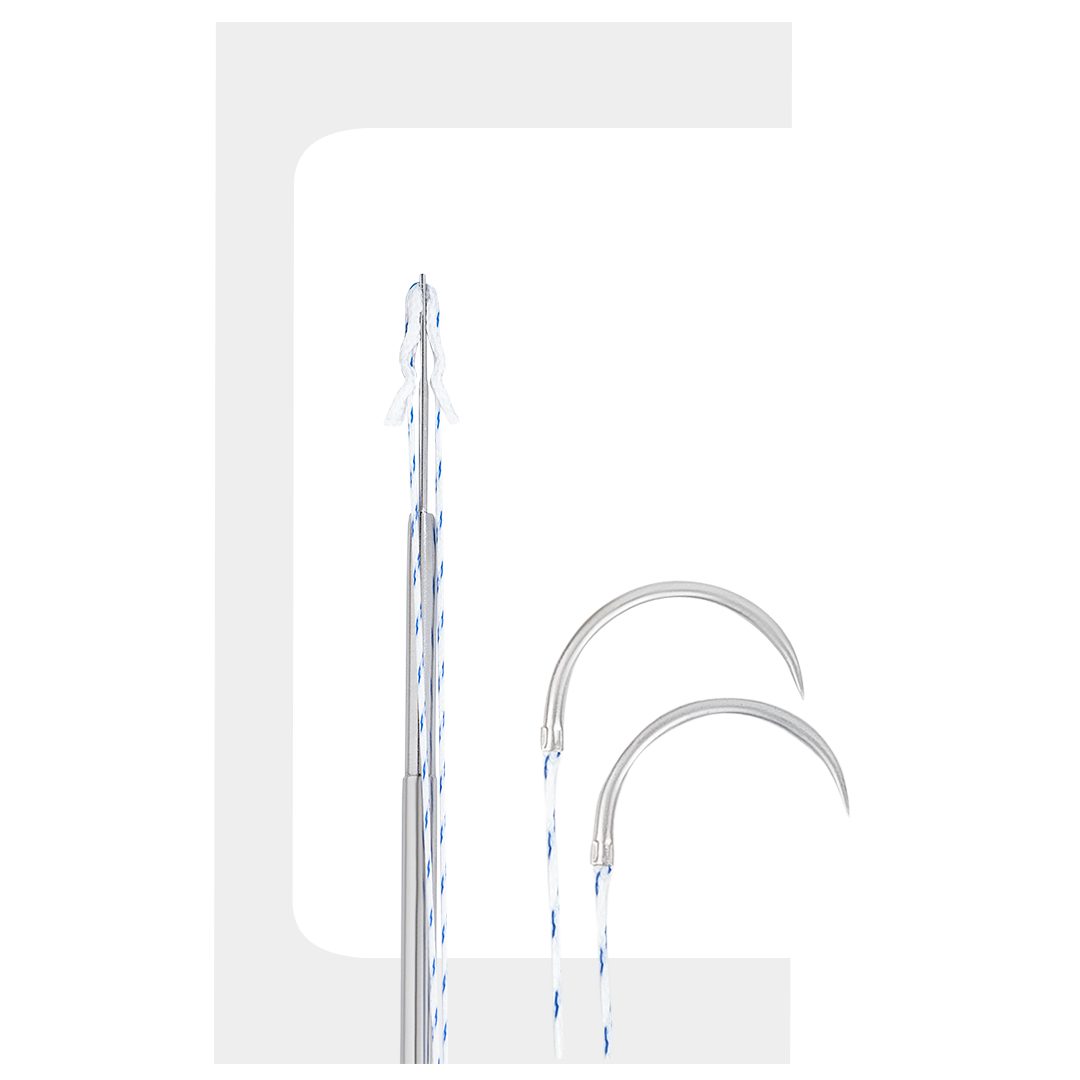
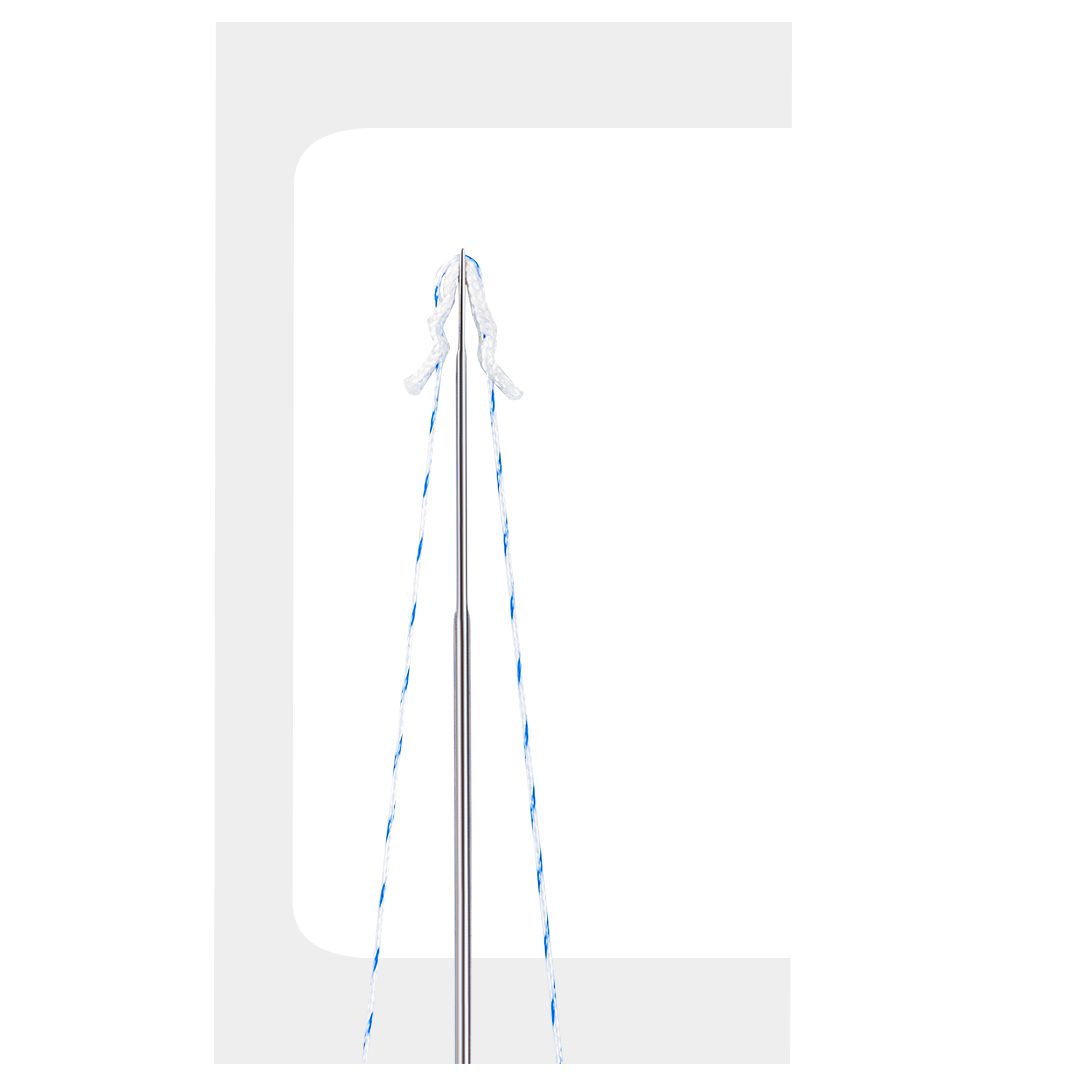
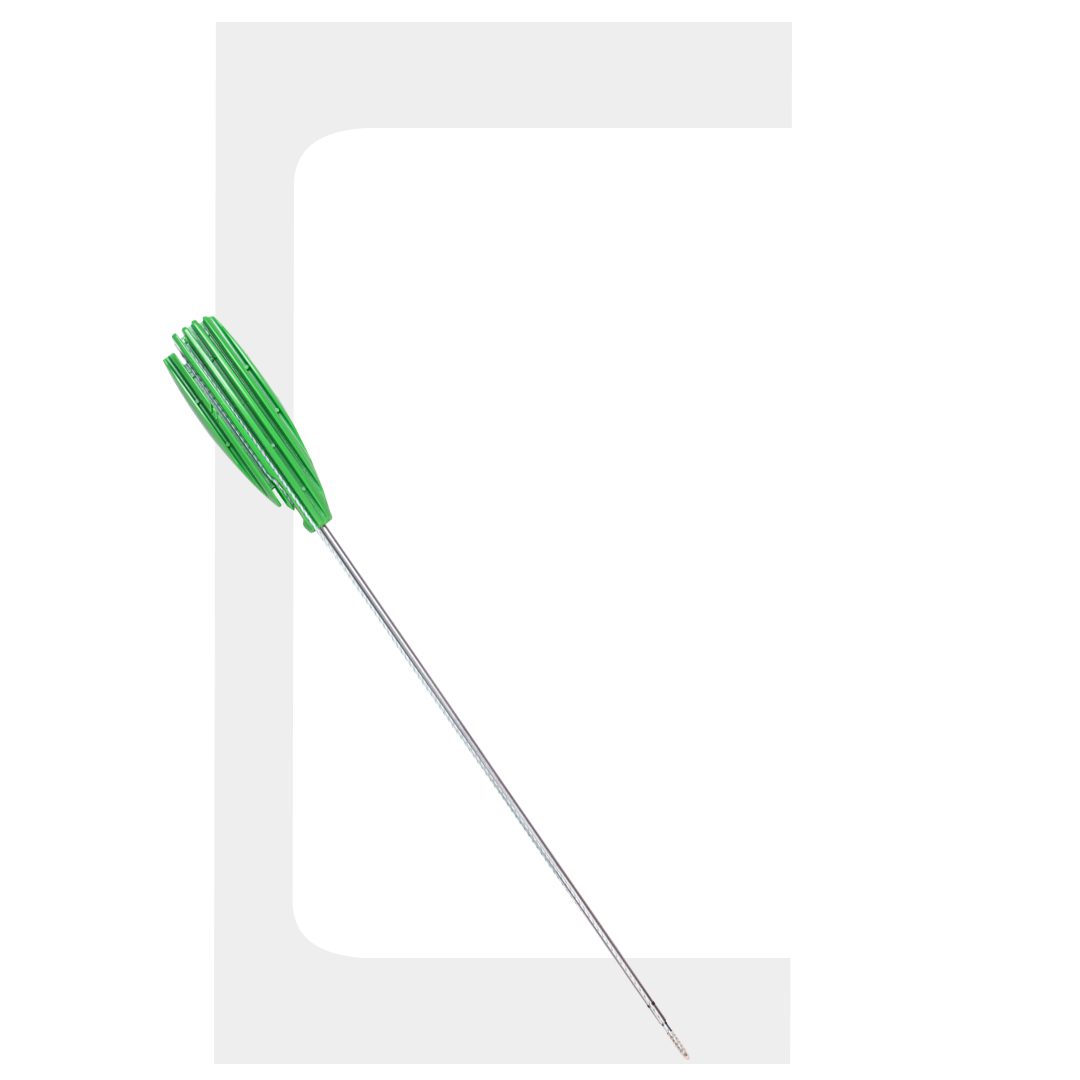
Suture anchors are the primary fixation devices in arthroscopic rotator cuff repair. They are inserted into the greater tuberosity, and sutures attached to the anchor are then passed through the tendon to reattach it to bone. Modern anchors are available in threaded, knotless, and vented configurations, in materials ranging from titanium to bioabsorbable polymers to bio-composite blends.
Anchor diameter, thread design, suture capacity, and insertion angle all affect pullout strength and the practicality of deployment in the confined subacromial space. Surgeons building their knowledge of shoulder arthroscopy essentials should evaluate each of these variables before committing to an anchor system for routine use.
Single-Row vs Double-Row Repair
Single-row repair uses one line of anchors placed medially at the articular margin. Double-row repair adds a second row of laterally placed anchors – often knotless – to recreate the full footprint of the supraspinatus tendon. Biomechanical studies consistently show that double-row constructs provide greater contact area and initial fixation strength, which is particularly relevant for larger tears and athletically active patients.
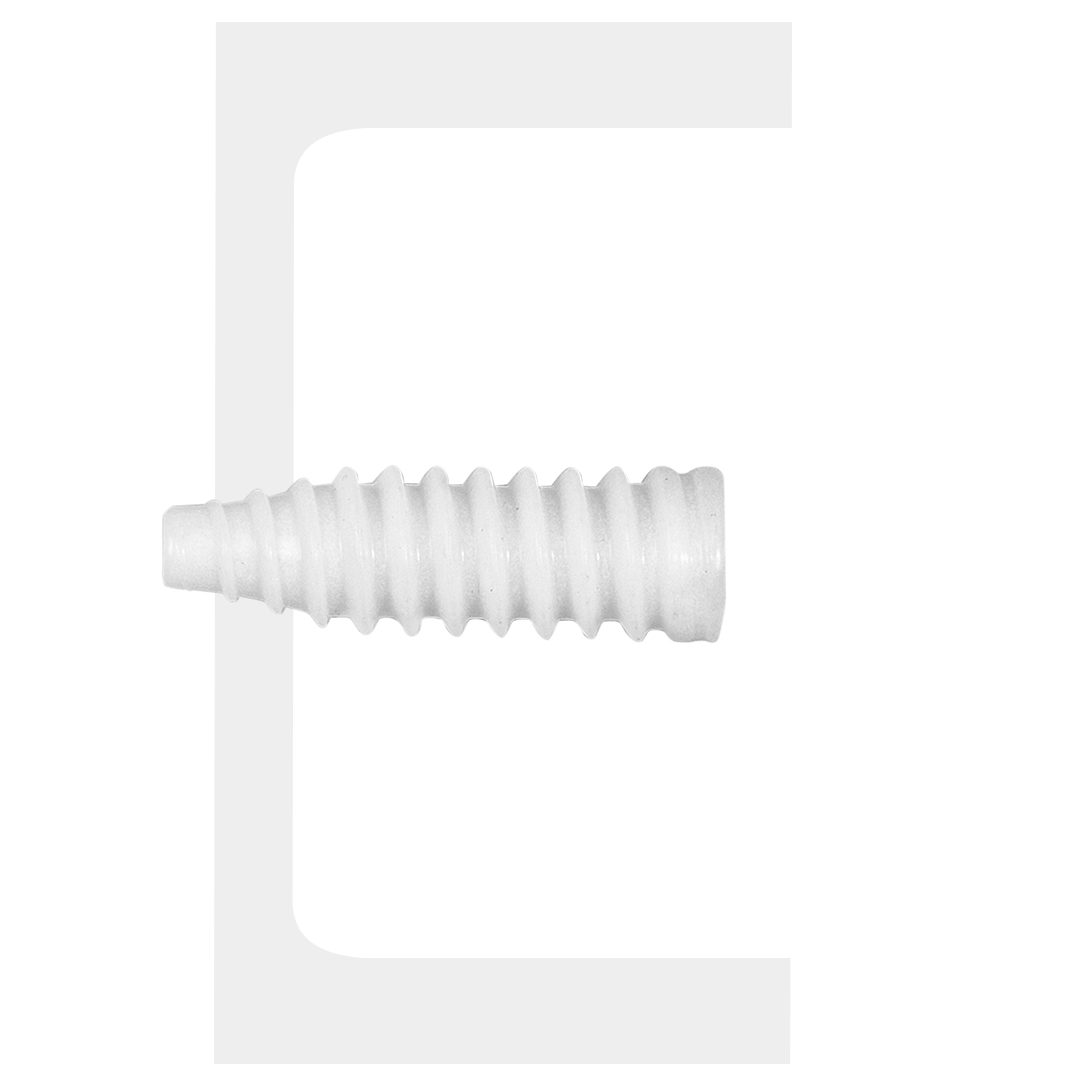
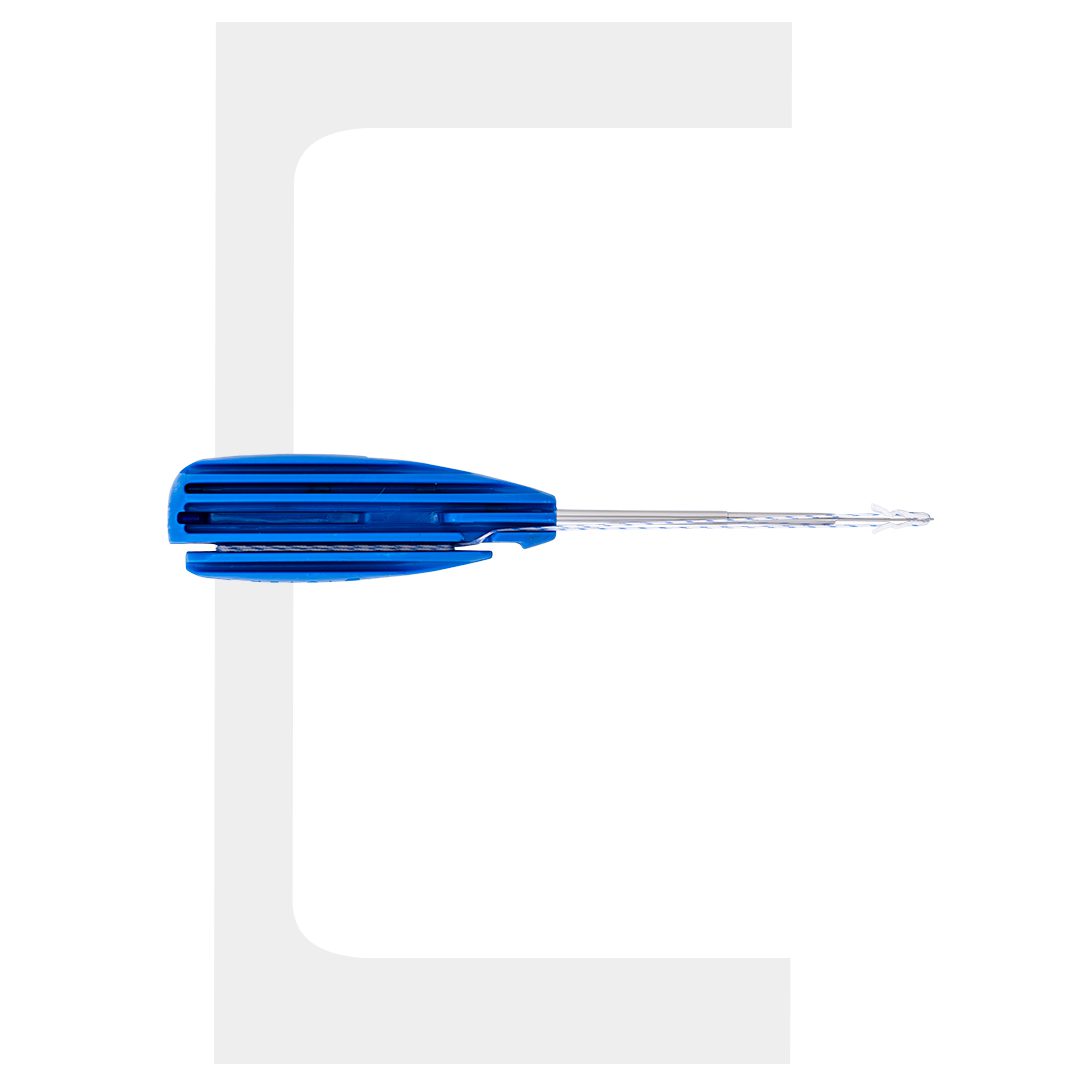
Knotless Anchors and All-Suture Designs
Knotless anchor systems – where the suture is tensioned and locked without arthroscopic knot tying – have significantly reduced operative time and eliminated knot-related complications such as knot impingement and suture abrasion. All-suture anchors, a newer design category, consist of a soft anchor body with a suture loop that locks under tension within the bone tunnel, offering a smaller insertion profile and preserving bone stock.
Biotek Arthroscopic Solutions for Rotator Cuff Repair
Among the implant systems available to surgeons today, Biotek arthroscopic implants for rotator cuff repair represent a clinically validated option designed around the demands of high-volume shoulder arthroscopy practice. Biotek arthroscopic solutions for rotator cuff repair include a range of anchor configurations – threaded and knotless, bioabsorbable and metal – matched with purpose-built arthroscopic shoulder instruments that integrate cleanly into standard portal setups.
Advanced arthroscopic rotator cuff repair with Biotek implants is supported by biomechanical testing data and a clinical track record across both single-row and double-row construct applications. The instrument-implant ecosystem is designed to reduce operative steps, provide consistent anchor seating feedback, and support reliable suture management throughout the repair sequence.
For surgical teams evaluating their implant inventory, the Biotek system offers a coherent platform rather than a collection of independently sourced components – a meaningful operational advantage in high-throughput arthroscopy units.
Shoulder Instability Repair: Beyond the Rotator Cuff
Rotator cuff repair is not the only indication for anchor-based fixation in the shoulder. Shoulder instability repair implants are used in Bankart reconstruction – reattachment of the anteroinferior labrum and inferior glenohumeral ligament complex following anterior dislocation – and in SLAP repairs involving the superior labrum and biceps anchor.
The anchor design requirements for labral repair differ slightly from cuff repair: smaller diameter anchors are often preferred at the glenoid rim to minimise bone disruption, and suture configuration must provide secure labral tissue capture without excessive bulk in the tight periglenoid space. Surgeons managing both cuff and instability pathology benefit from a system that covers both indications without requiring separate implant platforms.
Rotator Cuff Repair: Instruments & Implants at a Glance
| Tool / Implant | Function | Key Consideration |
|---|---|---|
|
Arthroscope (30-degree) |
Subacromial and GH joint visualization |
HD camera and light source essential |
|
Motorized Shaver |
Bursectomy and tendon edge prep |
Avoid over-resection of healthy tissue |
|
Burr |
Footprint decortication |
Creates vascularised bone bed for healing |
|
Suture Passer |
Tendon suture shuttling |
Accuracy determines mattress quality |
|
Threaded Anchor |
Primary tendon-to-bone fixation |
Pullout strength, suture capacity |
|
Knotless Anchor |
Lateral row, footprint compression |
Eliminates knot impingement risk |
|
All-Suture Anchor |
Minimally invasive fixation |
Preserves bone stock, small profile |
|
Instability Anchor |
Labral and SLAP repair |
Small diameter, periglenoid compatibility |
Frequently Asked Questions
1. What are the essential instruments for arthroscopic rotator cuff repair?
2. What is the difference between single-row and double-row rotator cuff repair?
3. What are shoulder instability repair implants used for?
4. How do Biotek arthroscopic implants support rotator cuff repair?
5. Are bioabsorbable anchors suitable for rotator cuff repair?
Conclusion
Rotator cuff repair is one of the most technically demanding and clinically rewarding procedures in shoulder arthroscopy. The outcomes patients achieve – pain relief, restored strength, and return to activity – depend directly on the quality of both the instruments used and the implants selected. From the initial bursectomy with the motorized shaver to the final anchor seating in a double-row construct, every step in the repair sequence is instrument- and implant-dependent.
Surgeons who invest in mastering shoulder arthroscopy essentials – including a thorough understanding of arthroscopic shoulder instruments, anchor biomechanics, and integrated solutions such as Biotek arthroscopic solutions for rotator cuff repair – are best positioned to deliver consistent, durable repairs. Whether managing rotator cuff pathology, shoulder instability, or labral injuries, a coherent, evidence-backed instrument and implant platform is the foundation every successful repair is built on.