Reliable Implants for Meniscus Surgery: What Surgeons Should Look For
Not all meniscus repair implants are created equal. With an expanding range of fixators, anchors, and suture-based constructs on the market, selecting the right device requires a clear framework. This article, drawn from a complete guide to meniscus repair, outlines exactly what surgeons should evaluate before committing to any implant system.
Why Implant Selection Matters
A meniscal tear repaired with the wrong implant – one that is poorly matched to tear geometry, tissue quality, or surgical technique – is significantly more likely to fail. Fixation failure means re-tear, repeat surgery, and in many cases, accelerated cartilage deterioration. Getting this decision right the first time protects both the patient and the repair.
What Makes an Implant Reliable?
Four core characteristics of meniscus surgery are: strong fixation, biological compatibility, ease of deployment, and independent clinical evidence.
1. Fixation Strength and Compression
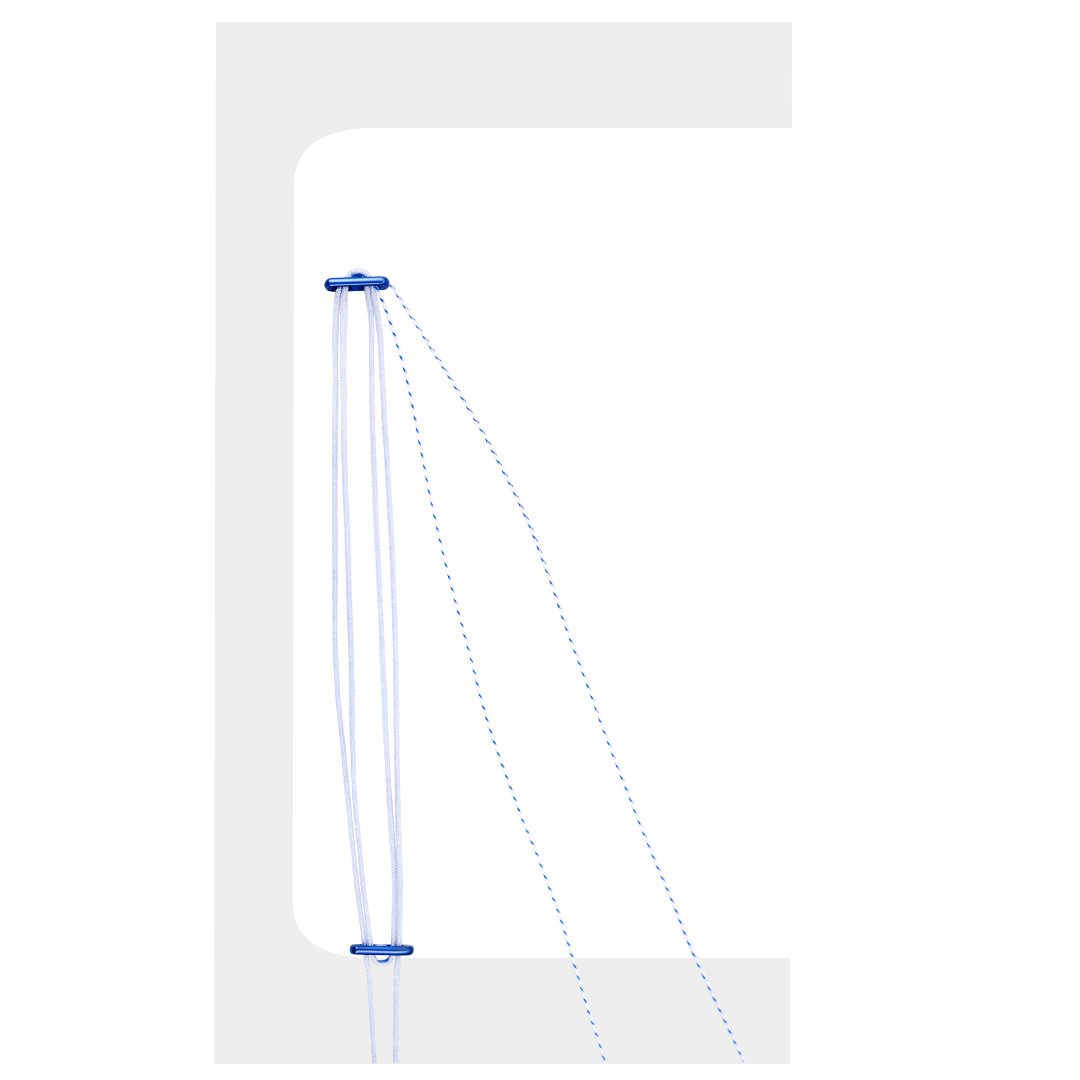
The implant must maintain compression at the repair site throughout the biological healing window – typically 12 to 16 weeks. Self-tensioning and cinch-lock mechanisms found in modern all-inside meniscus repair implants are designed to sustain this compression even as the surrounding tissue remodels. Weak or inconsistent fixation leads to gap formation and fibrocartilage healing failure.
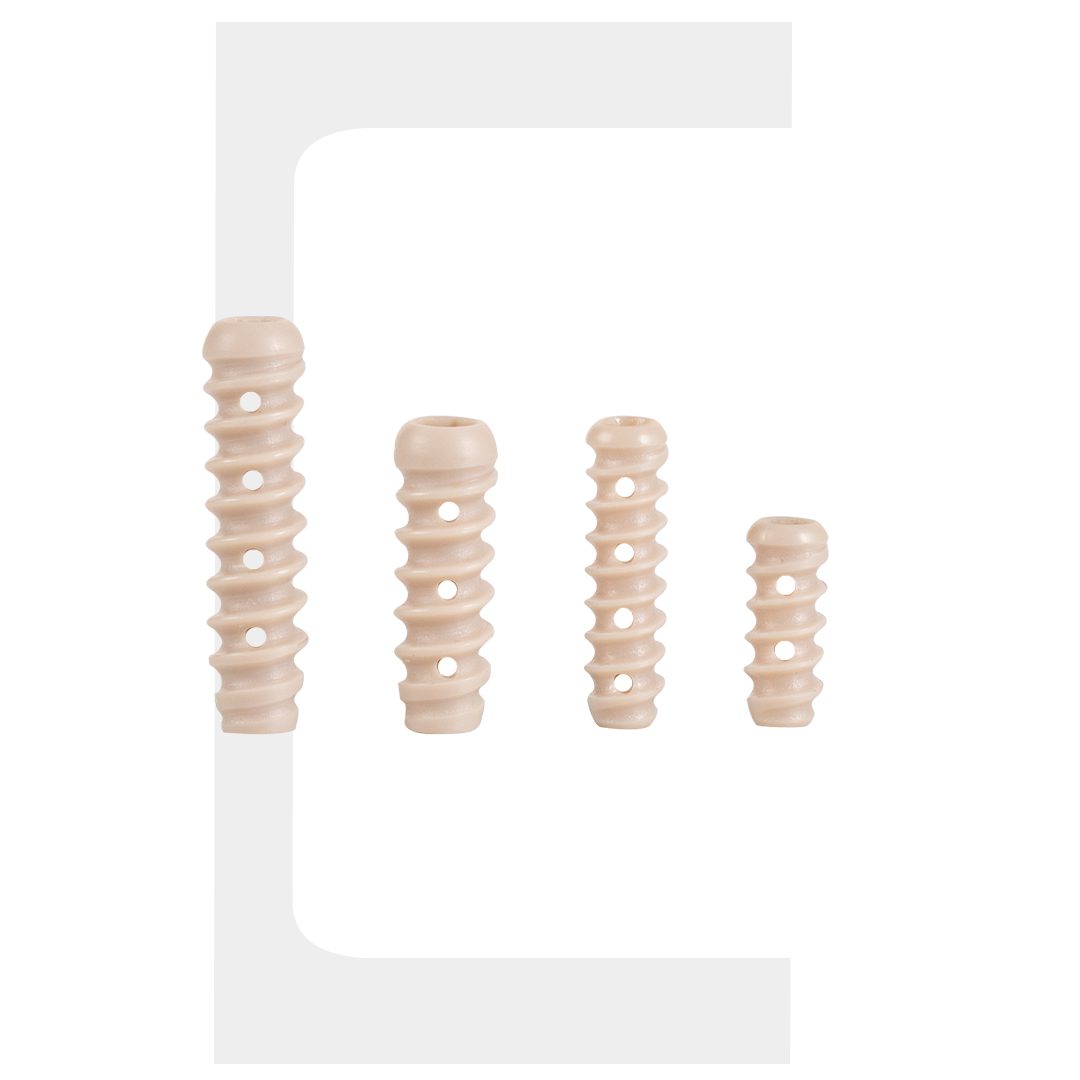
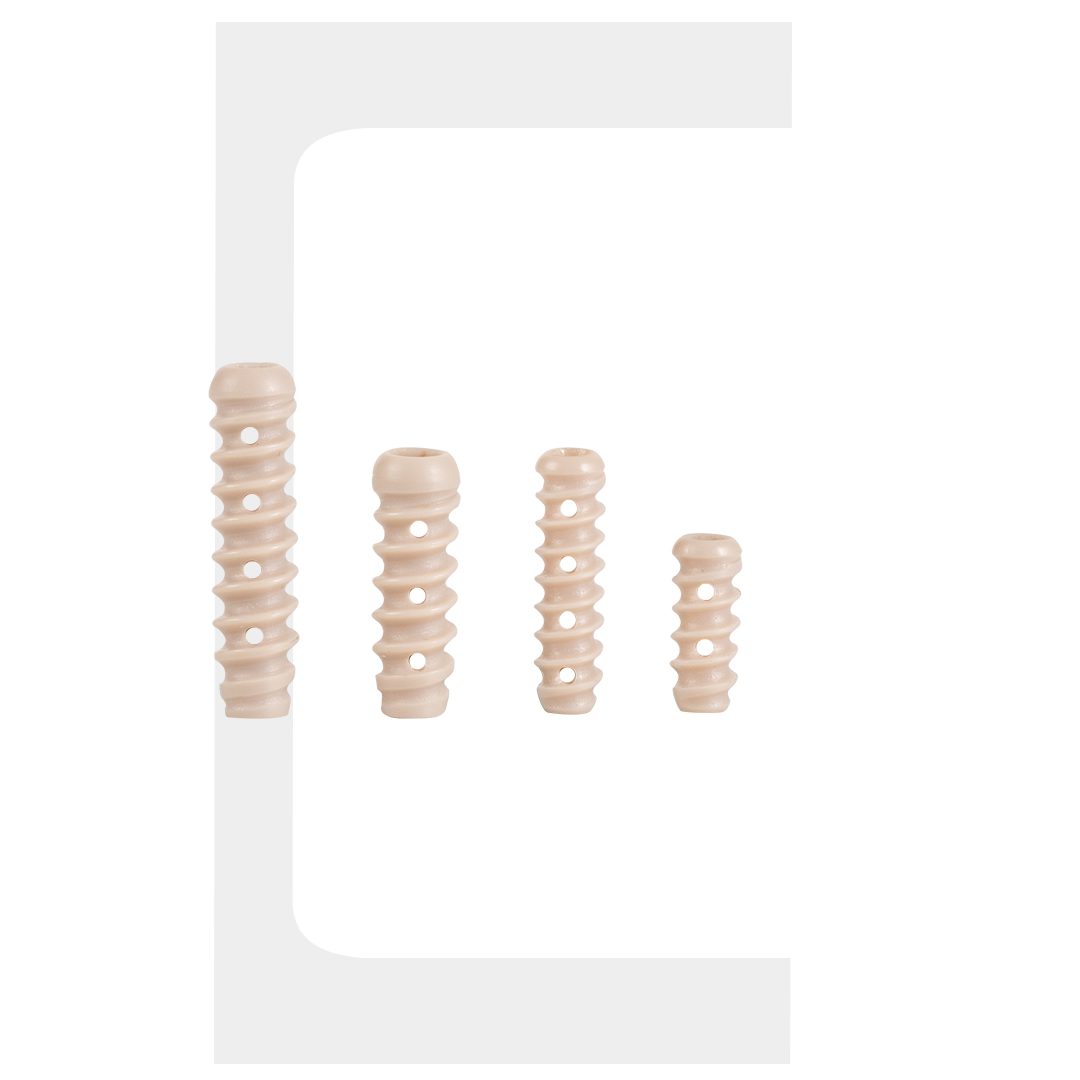
2. Material and Biocompatibility
Implant materials fall into three categories: bioabsorbable polymers (PLLA, PLGA), bio-composite blends, and permanent PEEK constructs. Bioabsorbable options gradually dissolve over 12 to 24 months, reducing long-term implant burden. Bio-composite materials resorb partially while encouraging tissue ingrowth. PEEK is non-absorbable and suited for high-demand fixation. The right material depends on patient age, activity level, and the specific meniscal repair system being used.
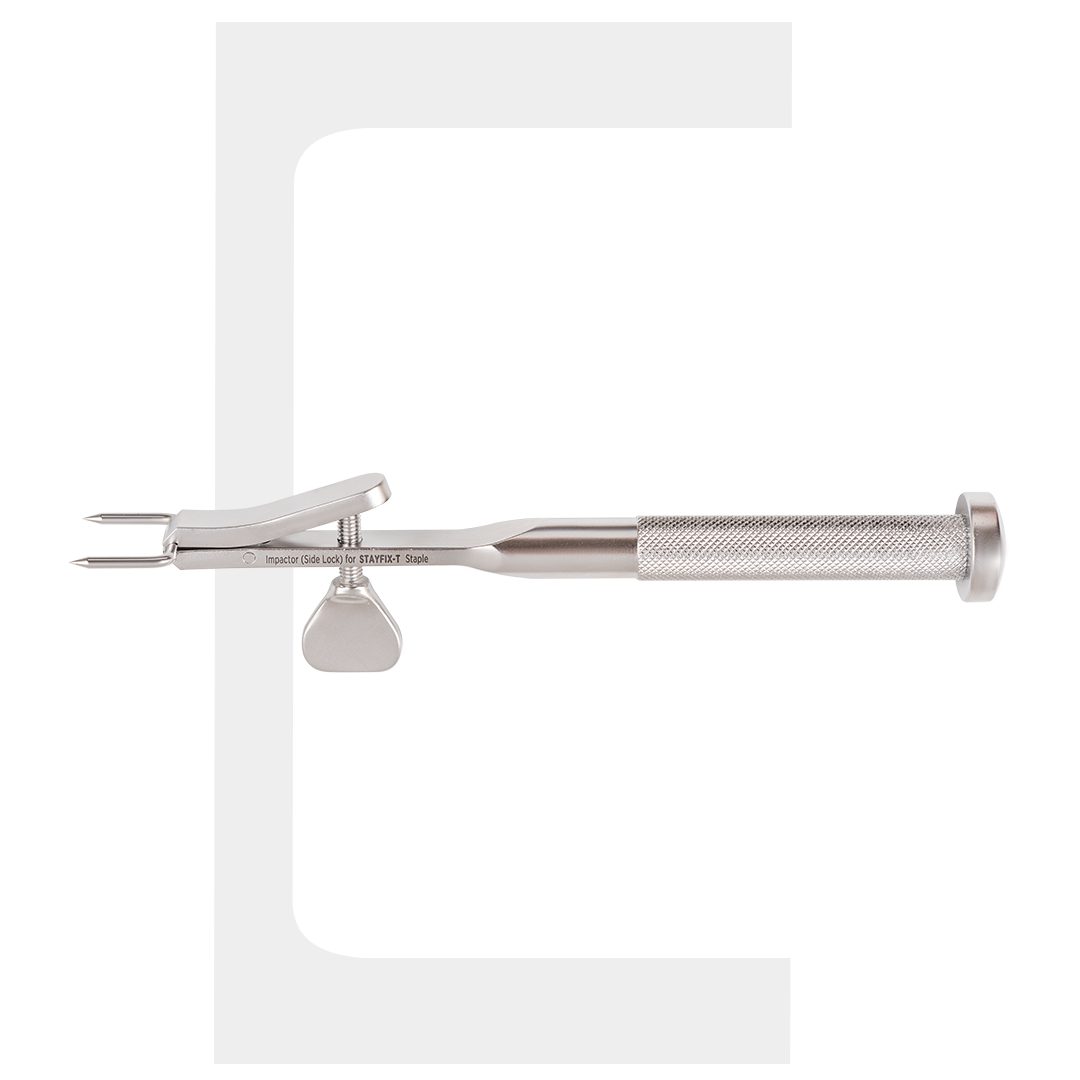
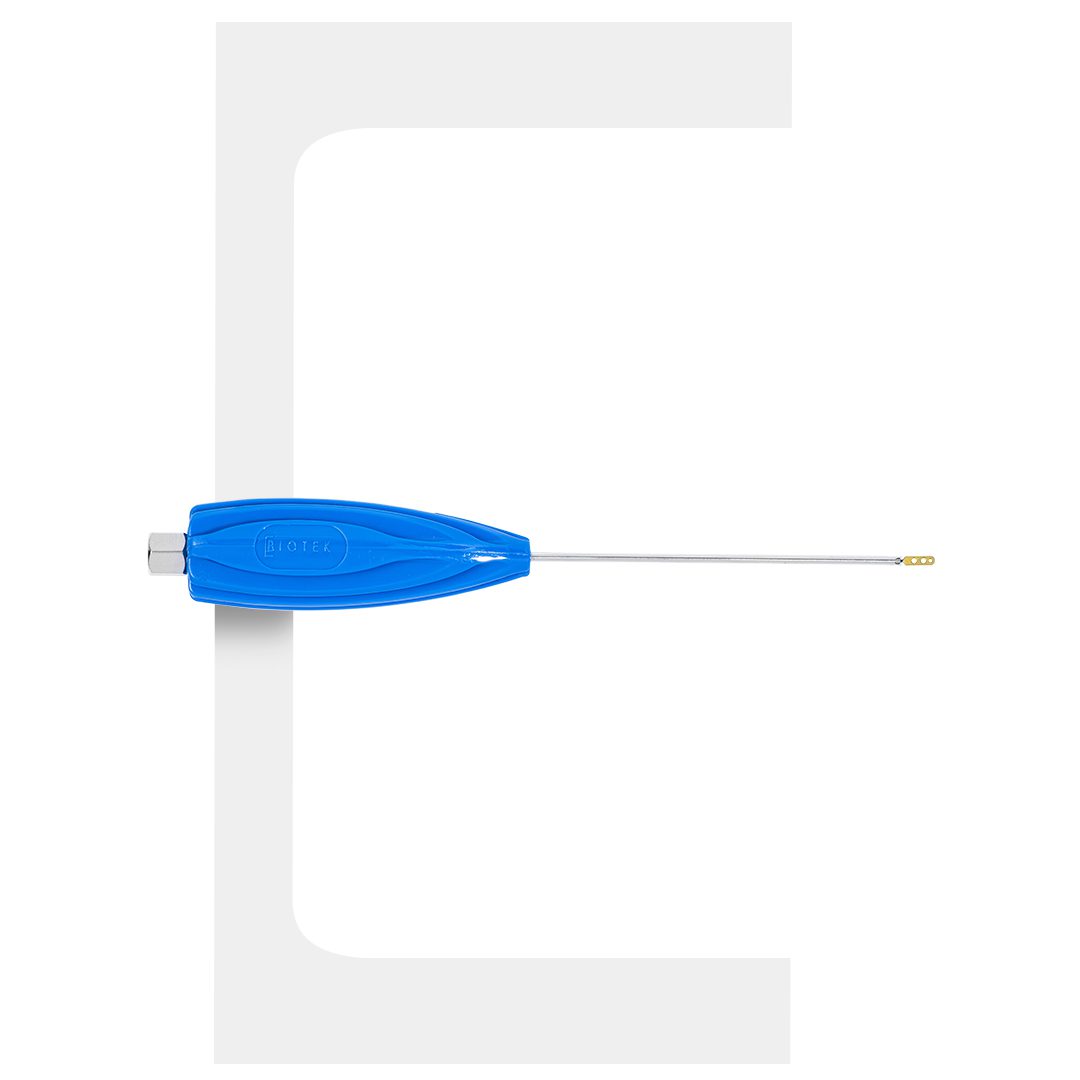
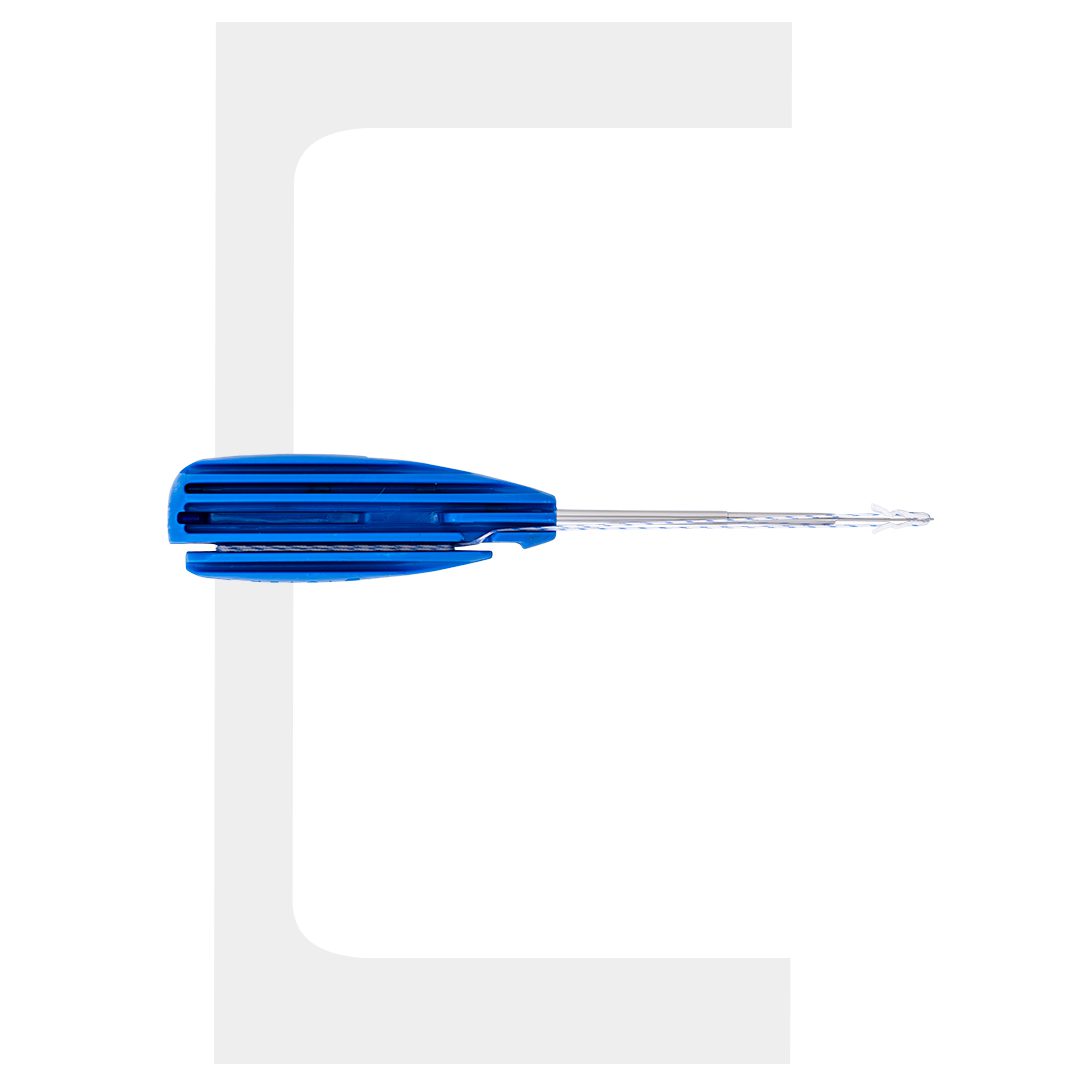
3. Instrument Compatibility
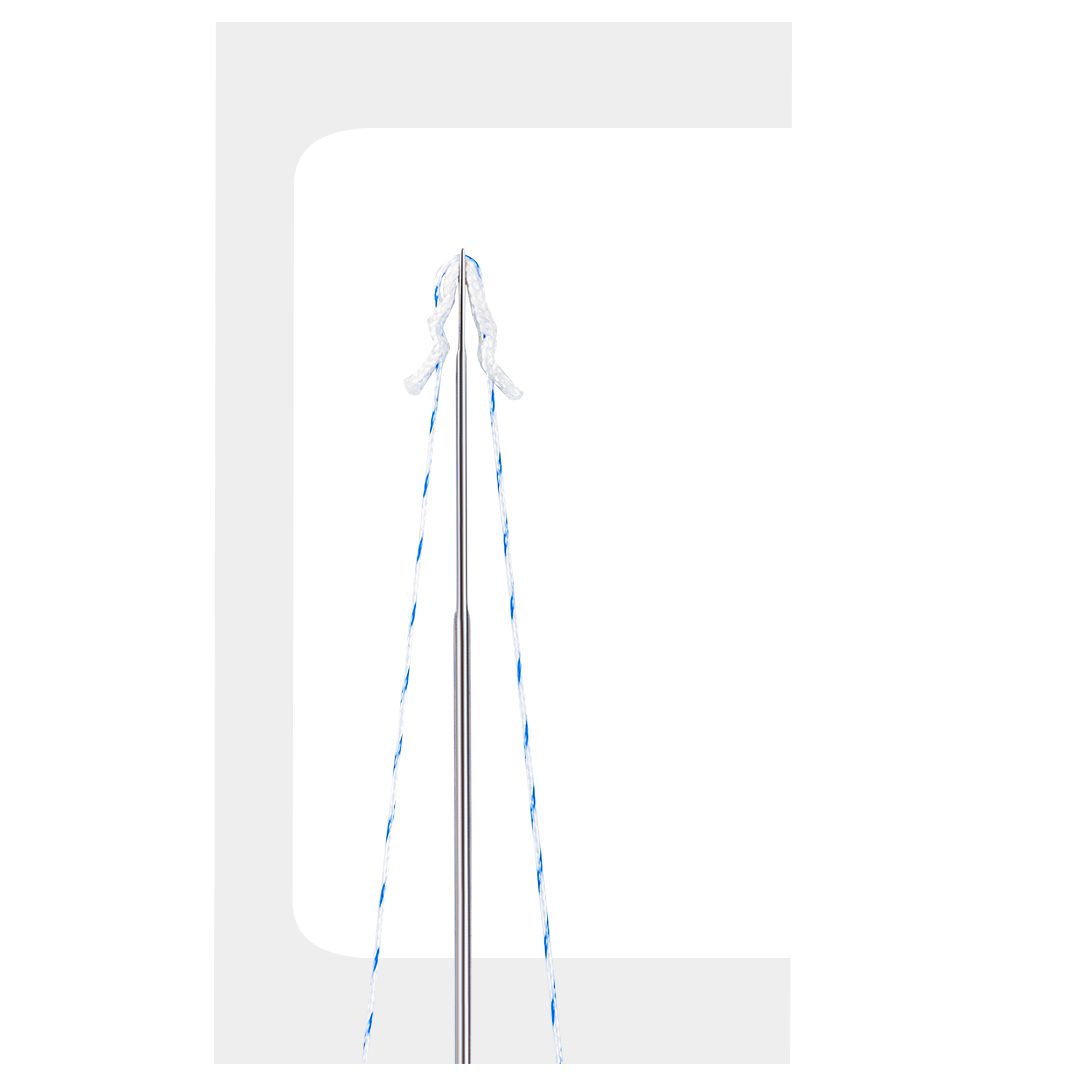
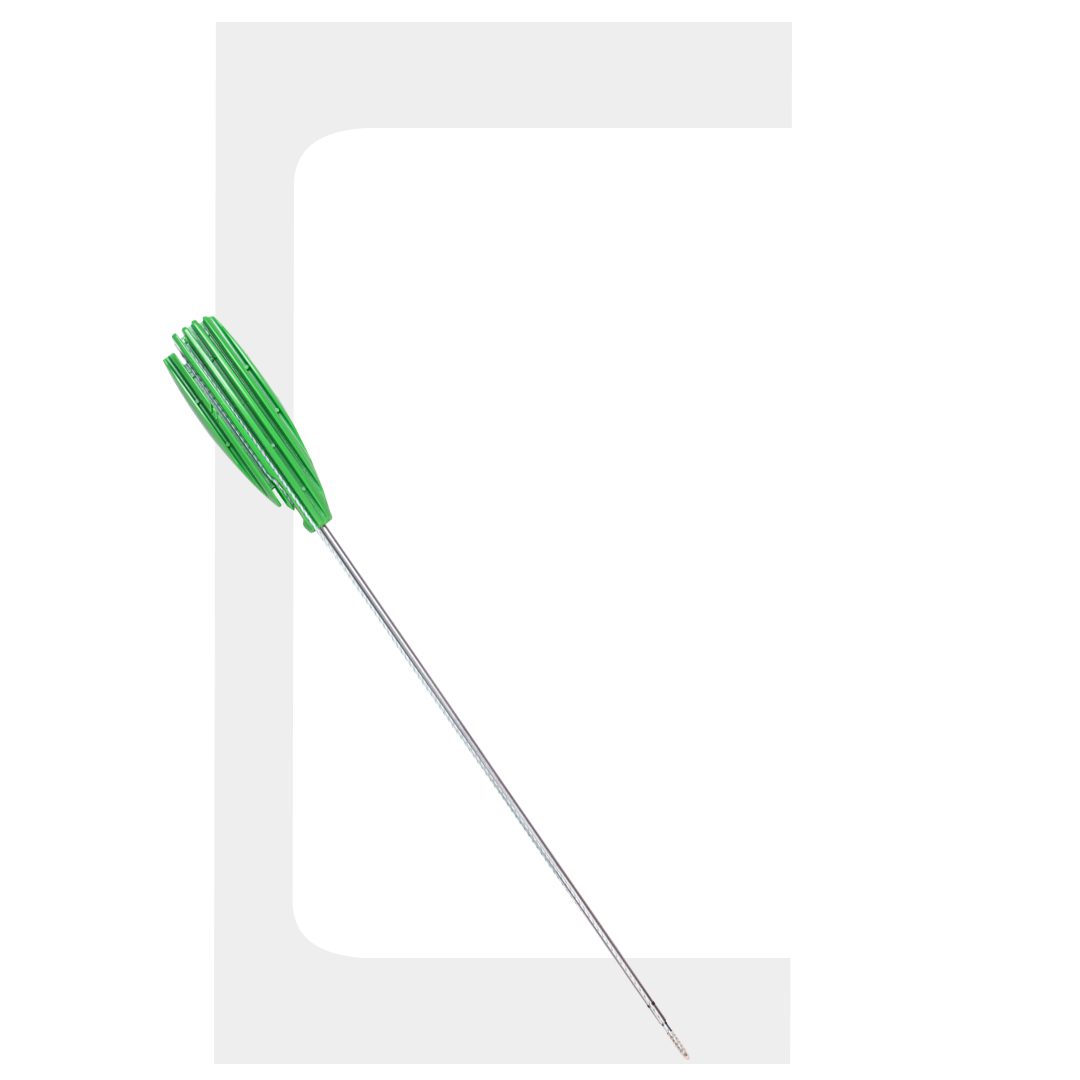
Even the best fixator underperforms if the deployment instrumentation is poorly designed. When evaluating meniscal repair systems, verify that the implant inserter fits standard arthroscopic portals without requiring additional incisions. The inserter should provide tactile feedback during anchor seating and allow accurate depth control in both medial and lateral compartments. Compatibility with instruments used for knee arthroscopy already in your inventory reduces operative complexity and cost.
4. Clinical Evidence
Implant reliability must be validated by independent peer-reviewed data – not manufacturer registries alone. Look for Level I or II studies reporting failure rates, functional outcome scores (IKDC, Lysholm, KOOS), and complication rates at minimum two-year follow-up. A fixator with strong biomechanical bench data but limited long-term clinical follow-up should be adopted cautiously.
Frequently Asked Questions
1. What are the most reliable implants for meniscus surgery?
All-inside bio-composite and bioabsorbable fixators with self-tensioning mechanisms currently have the strongest combination of clinical evidence and ease of use. Specific device selection should be guided by tear type, tissue quality, and the surgeon’s experience with the meniscal repair system.
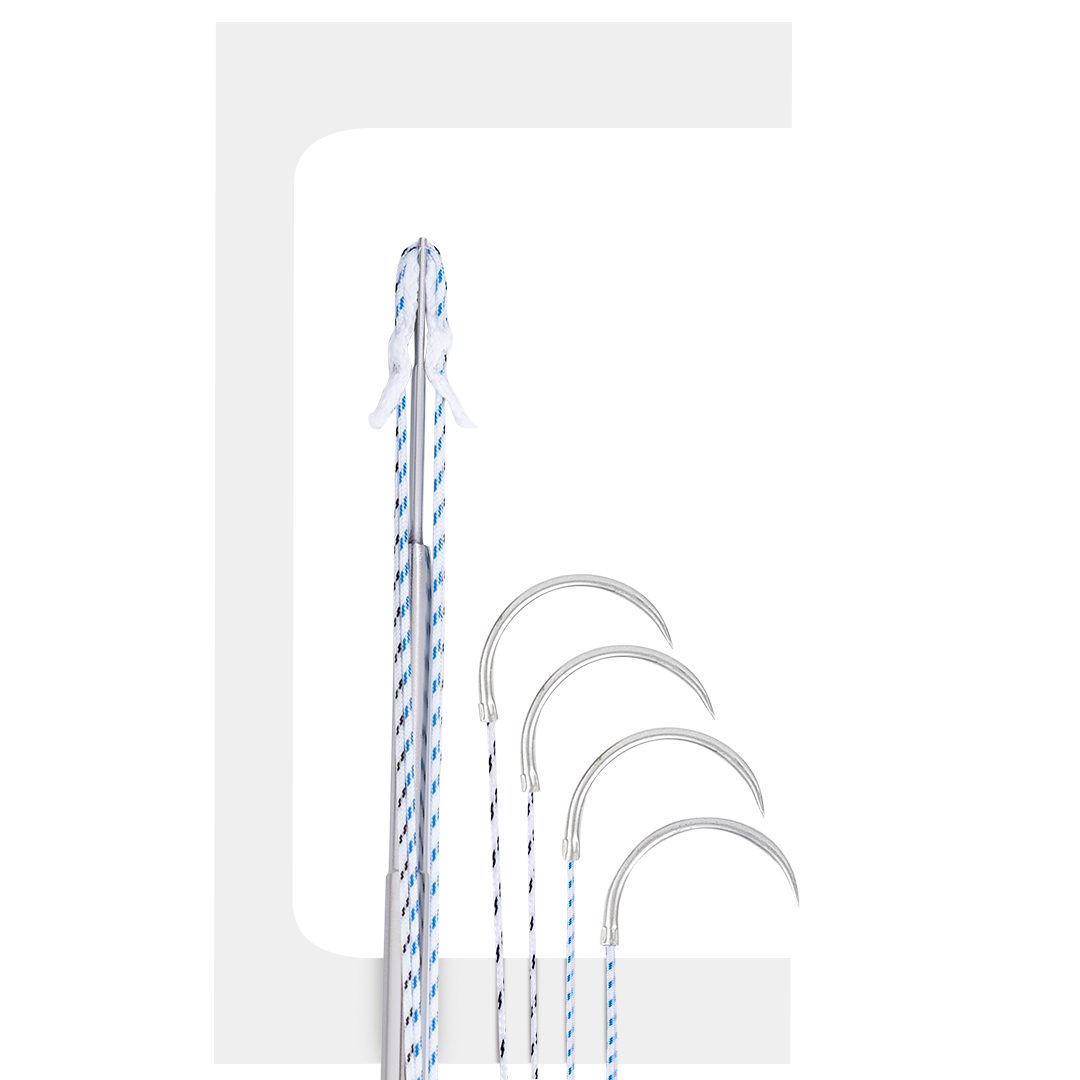
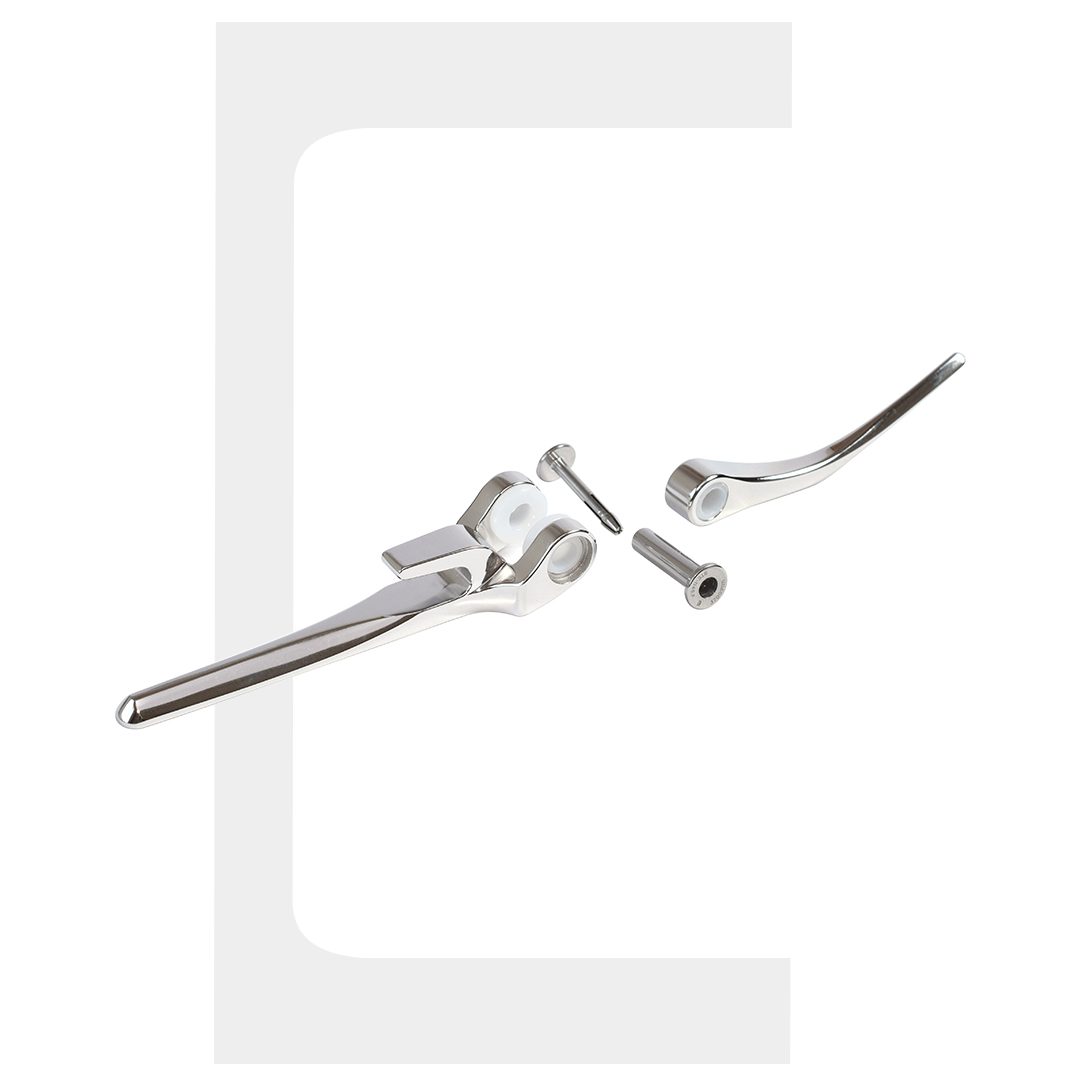
2. How do meniscus repair implants differ from suture-only repair?
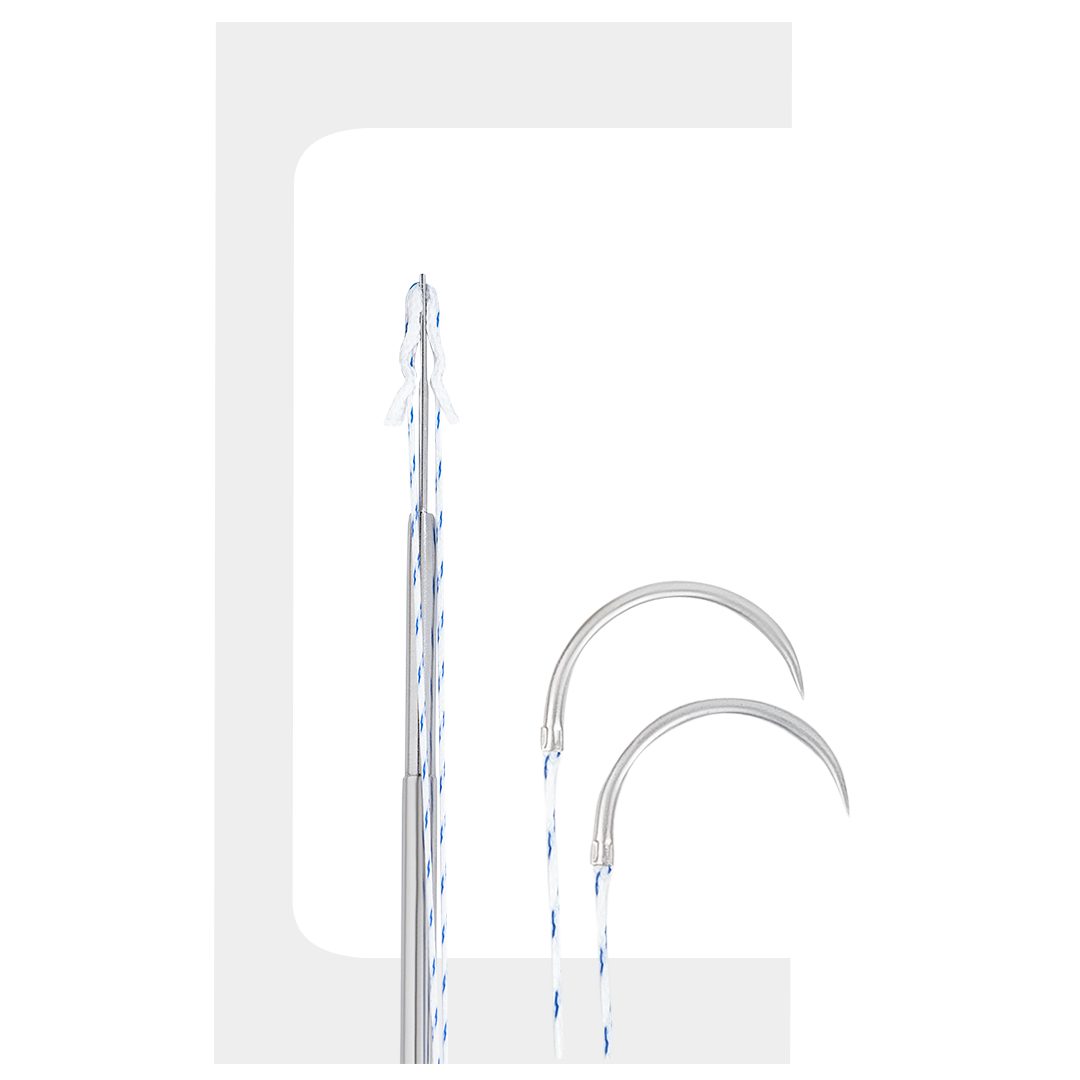
Dedicated meniscus repair implants – particularly all-inside fixators – eliminate the need for additional incisions and reduce neurovascular risk compared to inside-out suture techniques. They also offer controlled, reproducible tensioning that manual suture knots cannot consistently achieve.
3. Do implant materials affect recovery time?
Material choice influences the biological environment at the repair site but does not significantly change the overall rehabilitation timeline. Recovery is primarily driven by tear size, vascularity, and concurrent procedures such as ACL reconstruction.
4. Where do instruments used for knee arthroscopy fit into implant selection?
Instrumentation and implants should be evaluated together. The best meniscus repair implants are purpose-built with matched inserters that integrate cleanly into a standard arthroscopic workflow. A mismatch between implant and instrument adds operative time and fixation variability.
Conclusion
Choosing reliable implants for meniscus surgery comes down to fixation performance, material science, instrument compatibility, and clinical evidence. Surgeons who apply this framework – and who complement it with a complete guide to meniscus repair for deeper context on tear classification and patient selection – are best equipped to make consistent, evidence-based implant decisions that give their patients the best chance of durable healing.