5 Essential Skills Every Resident Must Master for Arthroscopic Proficiency
Arthroscopic surgery demands a unique combination of hand-eye coordination, spatial reasoning, anatomical fluency, and technical discipline that cannot be acquired from textbooks alone. For orthopedic residents entering this field, the early learning curve is steep – and the consequences of a poorly developed foundation show up not in exam scores, but in the operating room.
This article – drawn from educational authority perspectives in orthopedic surgeon education and training – identifies the five skills that most reliably separate residents who develop true arthroscopic proficiency from those who plateau. Whether you are a program director designing curriculum or a resident building your own development plan, these are the competencies that matter most.
Skill 1: Arthroscopic Spatial Orientation
The single most disorienting aspect of arthroscopic surgery for new residents is the disconnect between the two-dimensional monitor image and the three-dimensional joint space being navigated. Every instrument movement is indirect – the scope moves in the opposite direction to the image, and depth perception relies entirely on the surgeon’s mental map of the anatomy.
Developing reliable spatial orientation is the foundational skill in arthroscopic proficiency. Simulation-based training on box trainers and virtual reality platforms is now a recognised method for accelerating this skill within the education requirements for orthopedic surgeons, allowing residents to build their spatial map in a no-risk environment before applying it in live cases.
Programs built around competency-based training in arthroscopic procedures use objective metrics – instrument path efficiency, scope positioning time, and triangulation accuracy – to assess spatial orientation skill before advancing residents to more complex procedural steps.
Skill 2: Triangulation and Instrument Control
Triangulation – guiding a second instrument into the joint to meet the arthroscope’s field of view – is the core motor skill of arthroscopic surgery. It requires simultaneous control of two instruments through separate portals, coordination of bimanual movements, and the ability to adjust dynamically as the anatomy shifts with fluid pressure and patient positioning.
Poor triangulation technique leads to chondral scuffing, inadvertent tissue damage, and prolonged operative time. Education and training for orthopedic surgeons that includes structured triangulation exercises – initially on simulators, then on cadaveric specimens – consistently produces better intraoperative performance than unstructured case exposure alone.
Skill 3: Systematic Joint Diagnostic Assessment
Before any therapeutic intervention, the arthroscopist must complete a thorough, systematic diagnostic examination of the joint. In the knee, this means evaluating all three compartments; medial, lateral, and patellofemoral, in a consistent sequence. In the shoulder, it means surveying the glenohumeral joint and subacromial space with equal attention.
Residents who skip steps or perform incomplete diagnostic surveys miss pathology. Teaching a rigid, repeatable assessment protocol early in orthopedic surgeon education and training creates a habit that persists throughout a career. The diagnostic loop should be so ingrained that it runs automatically before therapeutic work begins.
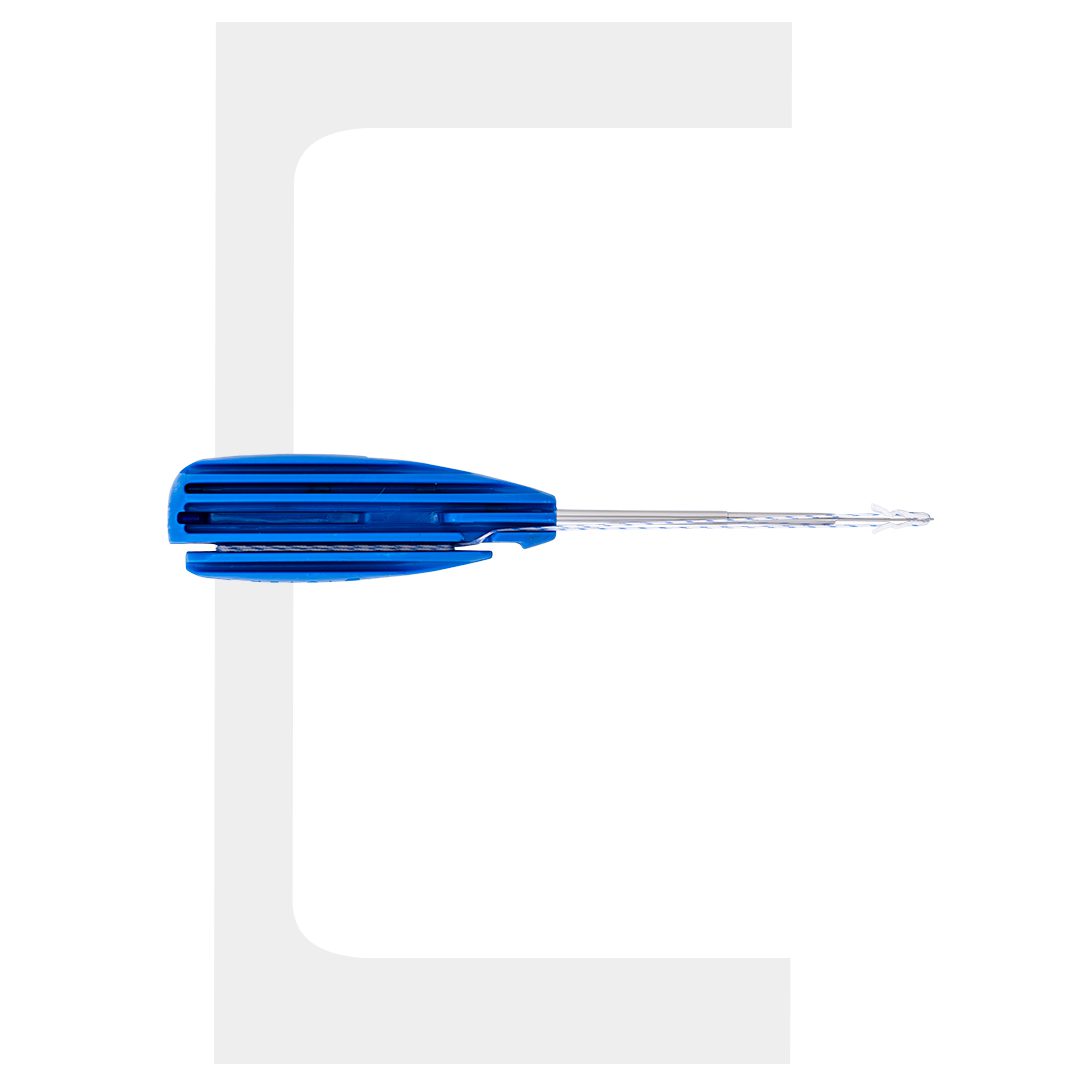
Skill 4: Suture Management and Knot Tying
Suture management is where arthroscopic technique meets constructive precision. In meniscal repair, rotator cuff fixation, and labral reconstruction, the ability to pass, retrieve, tension, and tie sutures under fluid in a confined space is what determines whether the construct holds or fails.
This skill has both a cognitive component – understanding which suture limb goes where in a multi-anchor construct – and a motor component that demands consistent hand mechanics. Surgical technician training programs that include structured suture-passing and knot-tying modules help prepare theatre teams to support surgeons efficiently, which in turn reduces operative time and cognitive load during the procedure itself.
Arthroscopic knot tying should be practiced to the point of automaticity. Residents who have to think through each step of a sliding knot under pressure are not ready to perform it in a live joint.
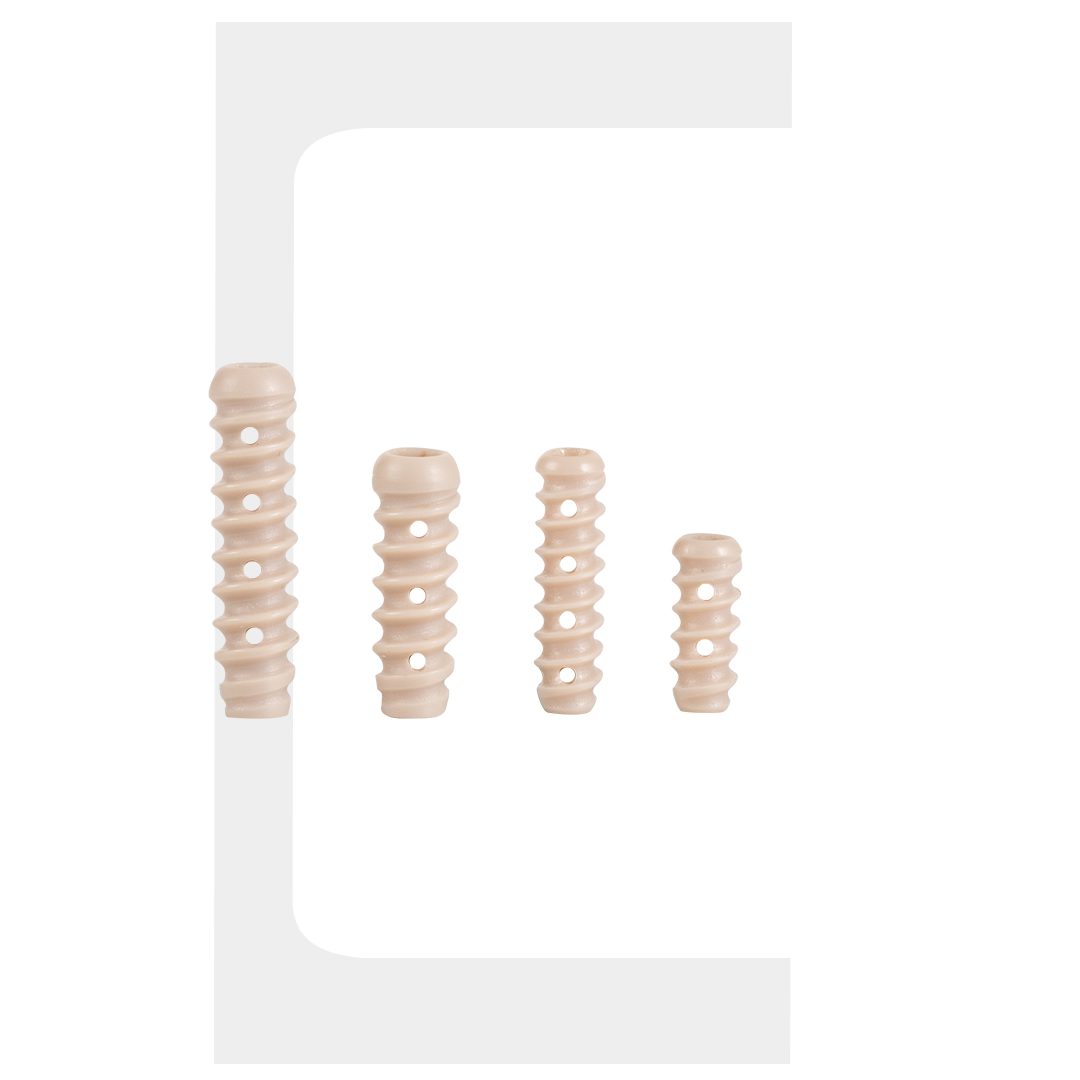
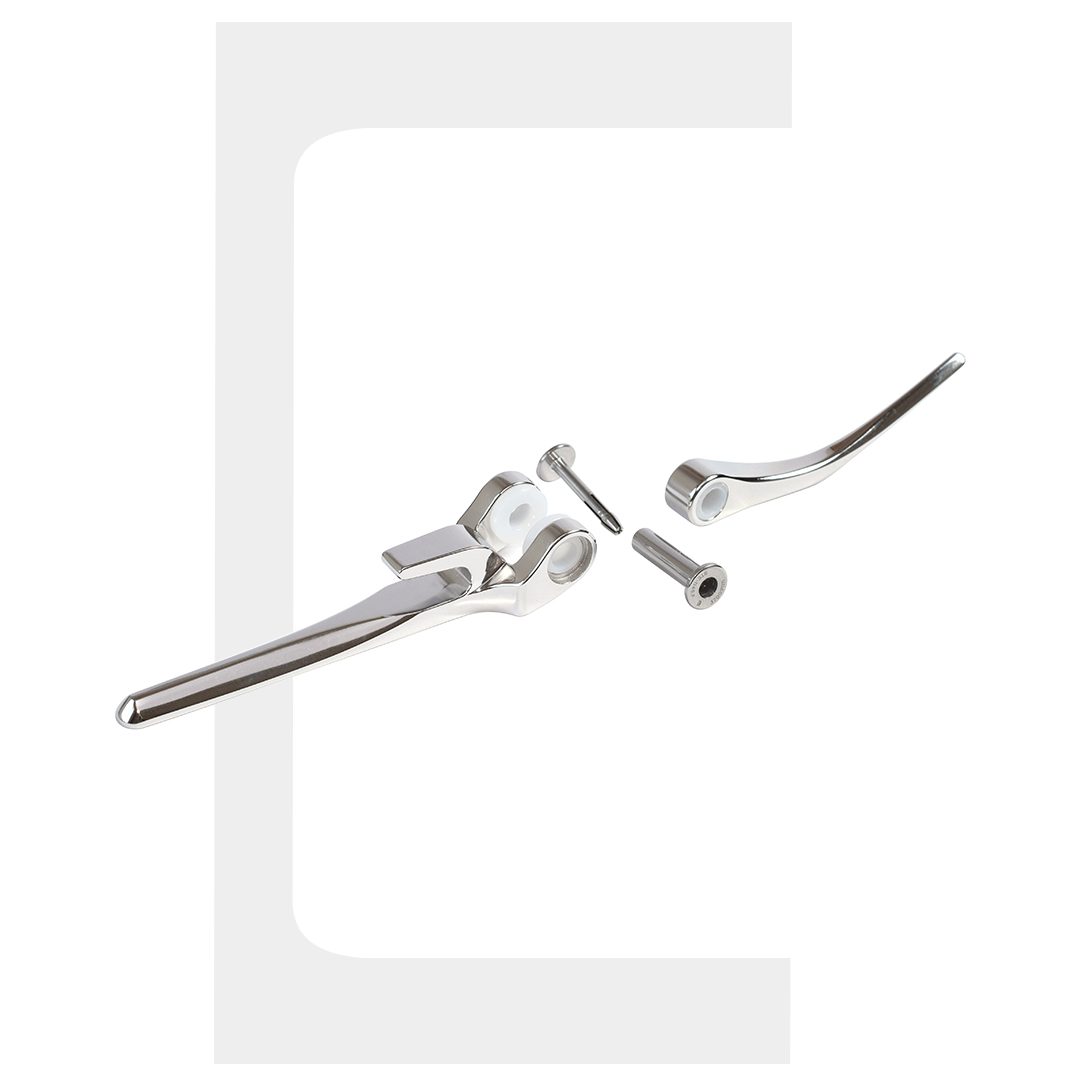
Skill 5: Implant Knowledge and Deployment Technique
Modern arthroscopy is implant-driven. Whether the procedure involves a suture anchor, a biodegradable fixator, or a meniscal repair device, the resident must understand the implant’s mechanism, deployment sequence, depth requirements, and failure modes before placing it in a patient.
This is an area where the education requirements for orthopedic surgeons increasingly extend beyond clinical training into device literacy. Residents should know how to assess whether an anchor is appropriately seated, recognise early signs of deployment failure, and manage intraoperative complications specific to the implant system being used.
Many leading orthopedic programs now incorporate manufacturer-supported simulation workshops and cadaveric implant labs as part of structured competency-based training in arthroscopic procedures, recognising that implant proficiency is a distinct skill set requiring dedicated practice.
Arthroscopic Training Skill Progression Framework
| Skill | Training Method | Competency Indicator |
|---|---|---|
|
Spatial Orientation |
Box trainer, VR simulation |
Consistent scope navigation without orientation loss |
|
Triangulation |
Simulator + cadaveric lab |
Accurate instrument-to-target without chondral contact |
|
Diagnostic Assessment |
Structured protocol repetition |
Complete joint survey in defined sequence, every case |
|
Suture Management |
Bench practice + theatre exposure |
Correct limb management and knot security under fluid |
|
Implant Deployment |
Cadaveric workshop + simulation |
Correct depth, position, and tension – first attempt |
Frequently Asked Questions
1. What are the education requirements for orthopedic surgeons specialising in arthroscopy?
2. How does competency-based training in arthroscopic procedures differ from traditional training?
3. What role do surgical technician training programs play in arthroscopy?
4. At what stage of residency should arthroscopic simulation training begin?
Conclusion
Arthroscopic proficiency is built skill by skill, not case by case. The five competencies outlined here – spatial orientation, triangulation, diagnostic assessment, suture management, and implant deployment – form the technical backbone of every successful arthroscopic surgeon. Programs that structure their education and training for orthopedic surgeons around explicit competency targets, supported by simulation, cadaveric practice, and structured surgical technician training programs for theatre teams, consistently produce residents who are better prepared for independent practice.
For residents reading this: identify which of these five skills is your current limiting factor. Then seek the specific training environment that addresses it directly. That targeted approach – not simply accumulating more cases – is what accelerates genuine arthroscopic mastery.